

If you intend to fill out delaware uc 1, you don't have to download any kind of applications - just make use of our PDF editor. Our editor is continually evolving to provide the very best user experience achievable, and that is thanks to our resolve for continuous improvement and listening closely to user feedback. For anyone who is looking to get going, this is what it takes:
Step 1: Click the "Get Form" button in the top area of this webpage to get into our tool.
Step 2: This tool offers the ability to change PDF files in a range of ways. Enhance it with personalized text, adjust what is originally in the PDF, and add a signature - all close at hand!
Filling out this PDF demands attentiveness. Make certain all mandatory areas are filled in accurately.
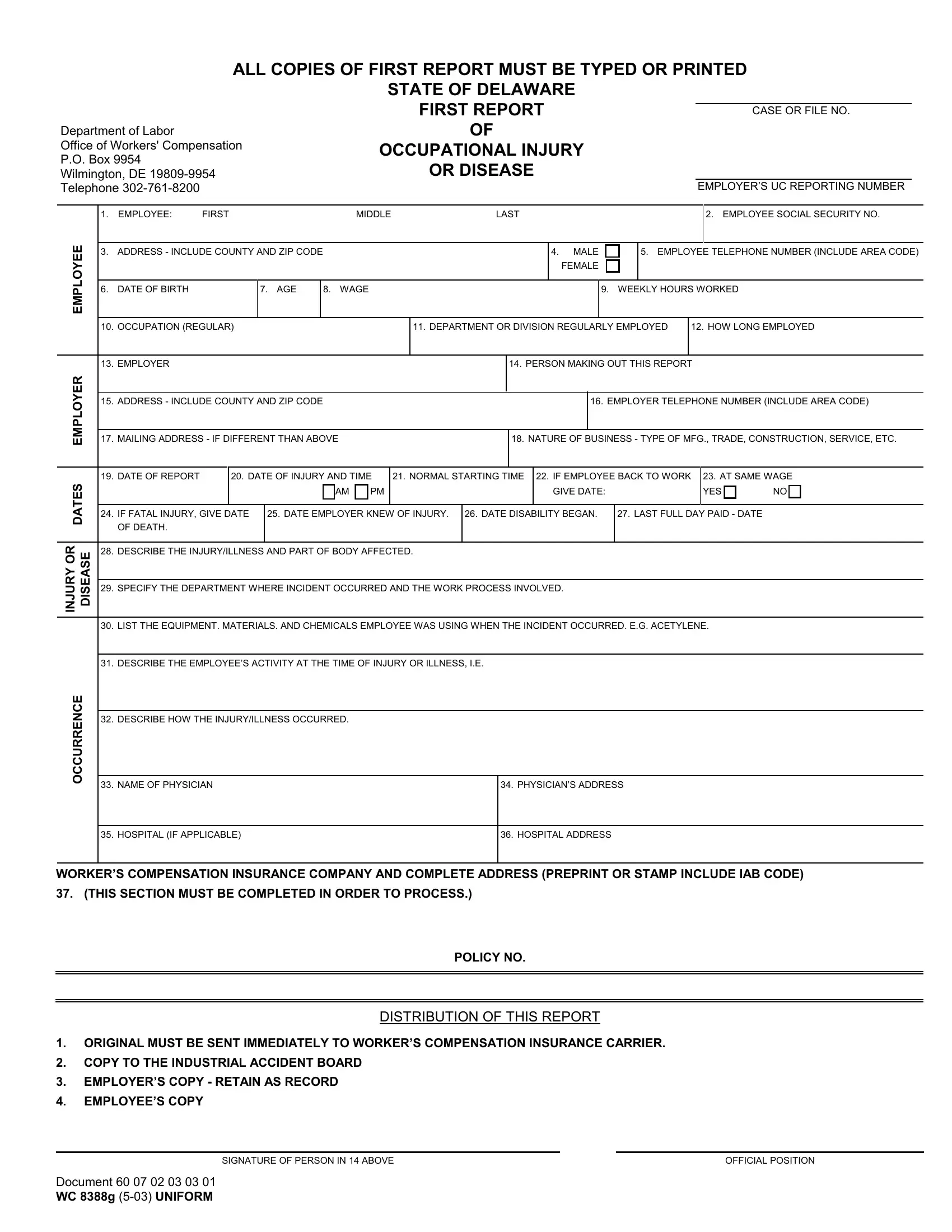
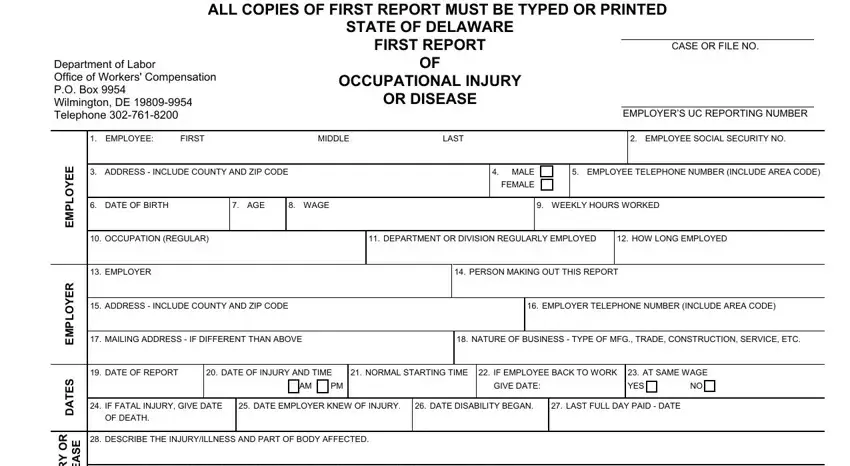
1. You'll want to complete the delaware uc 1 accurately, thus be attentive while filling out the segments including all of these blank fields:
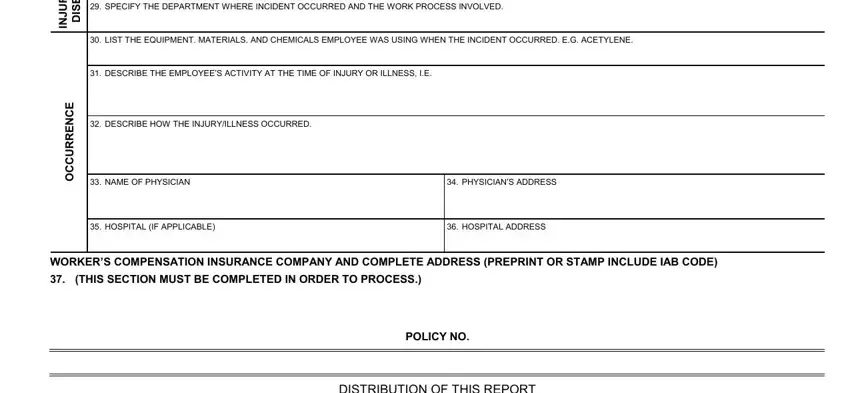
2. Just after performing the previous step, go on to the subsequent stage and fill out the essential details in these fields - R O Y R U J N, E S A E S D, SPECIFY THE DEPARTMENT WHERE, LIST THE EQUIPMENT MATERIALS AND, E C N E R R U C C O, DESCRIBE THE EMPLOYEES ACTIVITY, DESCRIBE HOW THE INJURYILLNESS, NAME OF PHYSICIAN, HOSPITAL IF APPLICABLE, PHYSICIANS ADDRESS, HOSPITAL ADDRESS, WORKERS COMPENSATION INSURANCE, THIS SECTION MUST BE COMPLETED IN, POLICY NO, and DISTRIBUTION OF THIS REPORT.
3. This subsequent segment is generally rather simple, EMPLOYEES COPY, Document WC g UNIFORM, SIGNATURE OF PERSON IN ABOVE, and OFFICIAL POSITION - all of these form fields has to be filled in here.

In terms of EMPLOYEES COPY and Document WC g UNIFORM, make sure you do everything right in this section. These two could be the key ones in this document.
Step 3: Proofread the information you have entered into the form fields and then hit the "Done" button. Find your delaware uc 1 when you subscribe to a free trial. Conveniently get access to the document in your personal account, together with any modifications and changes being automatically kept! FormsPal is devoted to the personal privacy of all our users; we always make sure that all personal data put into our system remains secure.