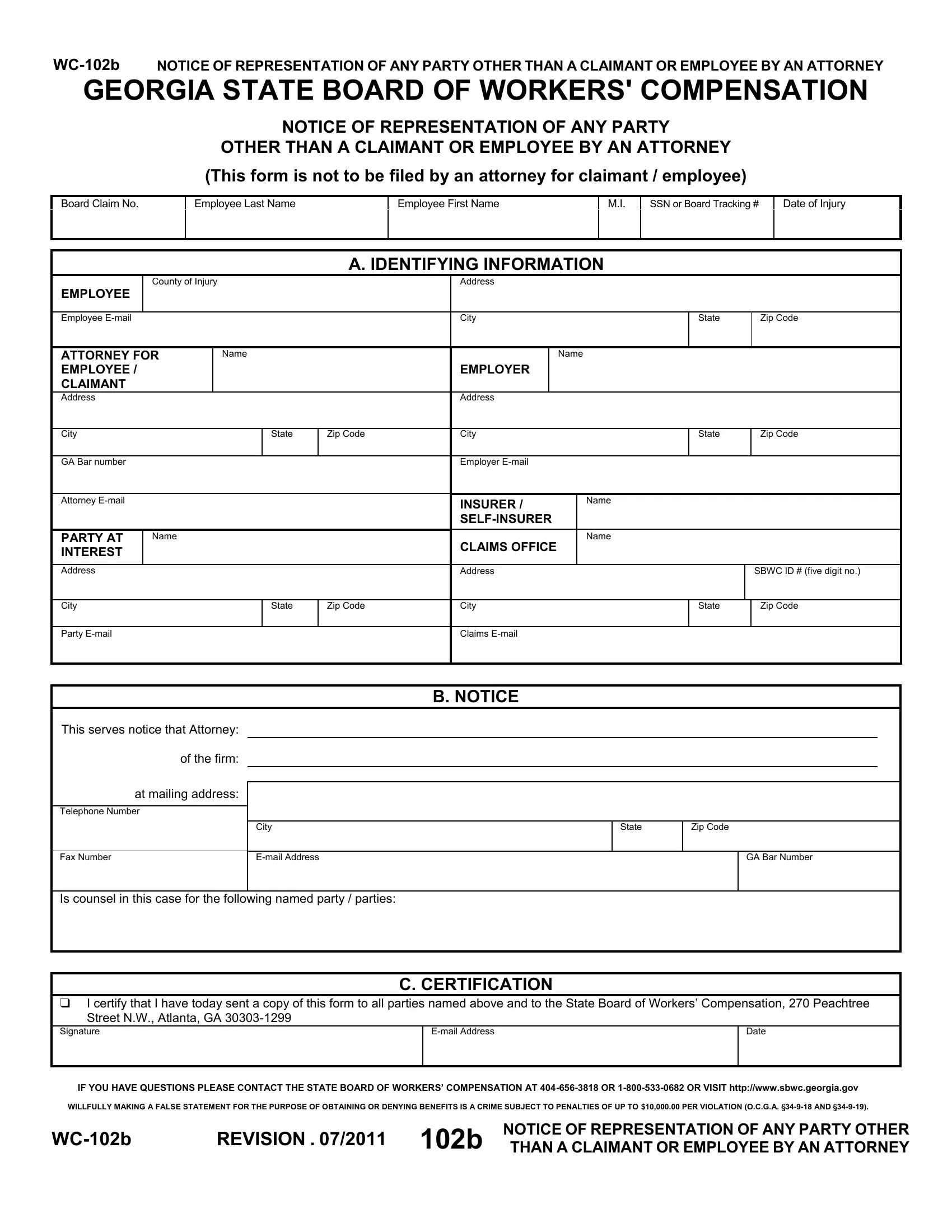
In Georgia, navigating the complexities of workers' compensation claims involves numerous steps and detailed processes, one of which includes proper notification when an attorney represents any party other than a claimant or employee. The WC-102b form, specifically designed by the Georgia State Board of Workers' Compensation, plays a critical role in this process. Its primary function is to notify the Board and all involved parties that an attorney is representing an entity other than an employee or claimant in a workers' compensation case. This could include employers, insurers, or self-insurers, among others. Essential parts of the form include identifying information about the employee, details of the attorney and the party they are representing, and a certification section that the attorney fills out to confirm the notice has been correctly distributed. The form also carries a caution against making false statements, highlighting the legal implications of such actions. Understanding the importance and correct use of the WC-102b form is essential for all stakeholders to ensure clear communication and adherence to Georgia's workers' compensation laws.
| Question | Answer |
|---|---|
| Form Name | Georgia Form Wc 102B |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | ga representation form, notice representation party attorney, georgia any party, georgia notice representation |