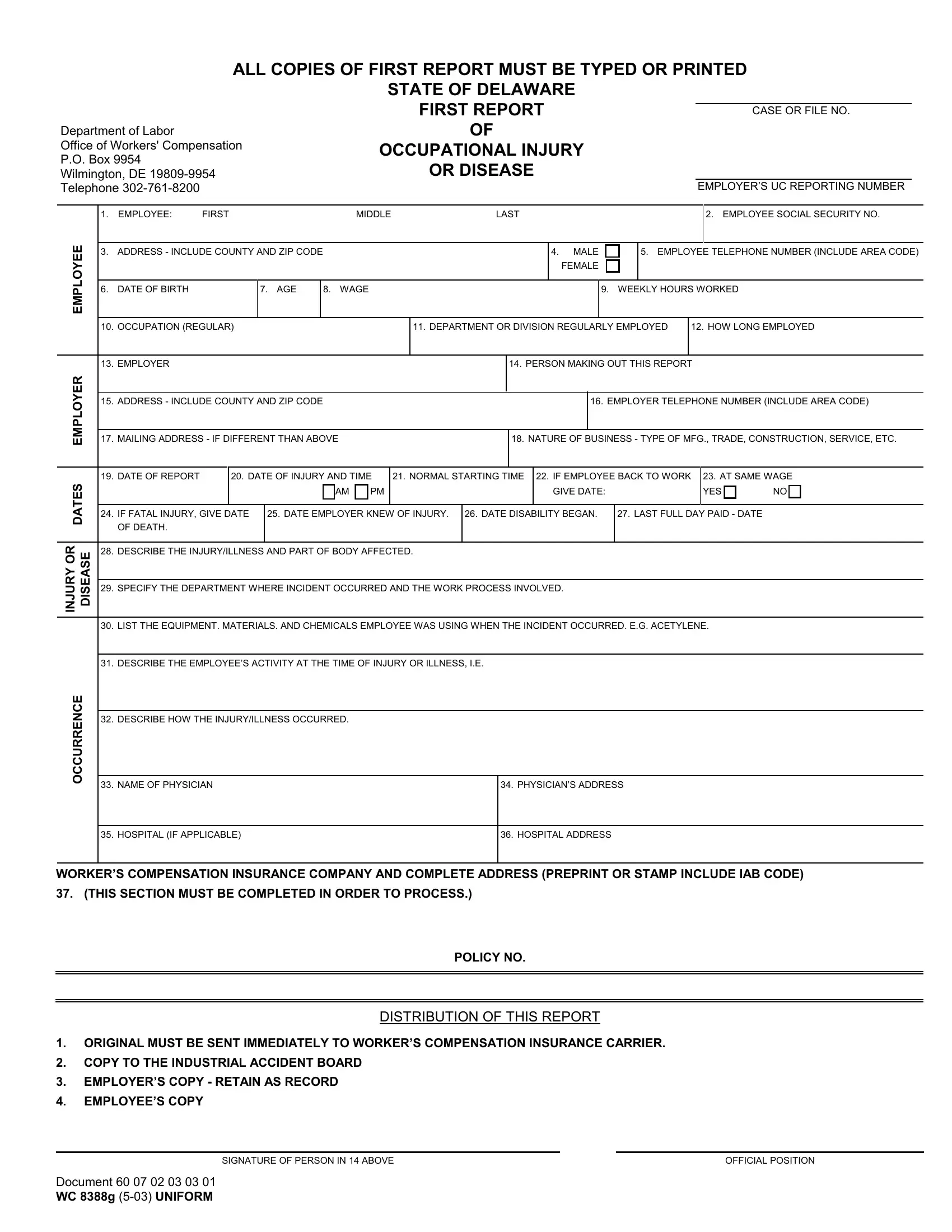
In the State of Delaware, navigating the complexities of workplace injuries requires a comprehensive understanding facilitated by specific documentation like the WC 8388G form. At the heart of the workers' compensation process, this form serves as the First Report of Occupational Injury or Disease, ensuring that all pertinent details about the incident are meticulously recorded and communicated to relevant parties. From employer details to the intricate specifics of the injury and the circumstances under which it occurred, the form is structured to capture a wide range of data including, but not limited to, the employee's personal information, the nature of the injury or disease, and the treatment provided. Moreover, it outlines critical steps for both employer and employee post-accident, advocating for expedited medical treatment, accurate record-keeping, and timely communication with Delaware's Office of Workers' Compensation. Such rigorously detailed documentation is indispensable for facilitating the claims process, determining compensation eligibility, and ultimately, ensuring the injured or ill employee receives the necessary support and benefits. The WC 8388G form is thus a crucial tool within the workers' compensation framework, symbolizing the Delaware Department of Labor’s commitment to protecting workers while fostering a transparent and efficient pathway to recovery and compensation.
| Question | Answer |
|---|---|
| Form Name | Form Wc 8388G |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | 8388g, form, uc1 delaware, uc-1 |