In the realm of sleep disorder diagnosis and management, the WH1220 form plays a pivotal role. Originating from Winchester Hospital's Sleep Disorders Center in Massachusetts, this comprehensive document facilitates the efficient and accurate collection of patient information critical to assessing and treating sleep-related issues. The form serves as a conduit between referring physicians and sleep specialists, ensuring that every patient receives tailored care based on their unique symptoms and medical history. By covering an array of conditions from Obstructive Sleep Apnea (OSA) to narcolepsy, and specifying the type of sleep study required, it meticulously outlines the pathway towards diagnosis. Moreover, the form allows for the integration of patient preferences and medical necessities, such as CPAP titration or the need for special accommodations. With sections dedicated to capturing detailed patient data, including medical history, primary symptoms, and current medications, the WH1220 form embodies a critical step in the journey towards restorative sleep and overall well-being.
| Question | Answer |
|---|---|
| Form Name | Form Wh1220 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | Sleep_Evaluatio n_Form winchester hospital sleep disorder center form |
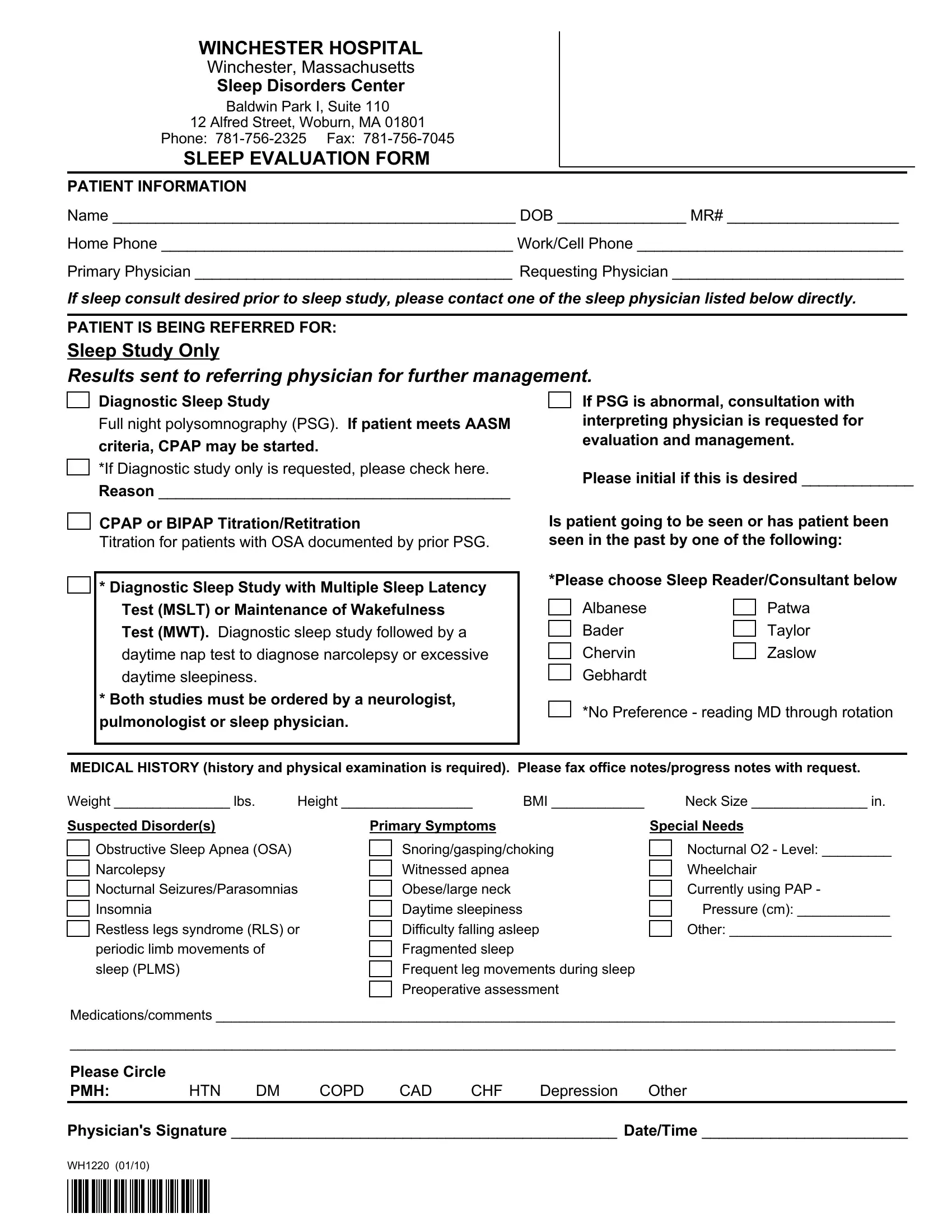
WINCHESTER HOSPITAL
Winchester, Massachusetts
Sleep Disorders Center
Baldwin Park I, Suite 110
12 Alfred Street, Woburn, MA 01801
Phone:
SLEEP EVALUATION FORM
PATIENT INFORMATION
Name _______________________________________________ DOB _______________ MR# ____________________
Home Phone _________________________________________ Work/Cell Phone _______________________________
Primary Physician _____________________________________ Requesting Physician ___________________________
If sleep consult desired prior to sleep study, please contact one of the sleep physician listed below directly.
PATIENT IS BEING REFERRED FOR:
Sleep Study Only
Results sent to referring physician for further management.
Diagnostic Sleep Study
Full night polysomnography (PSG). If patient meets AASM
criteria, CPAP may be started.
*If Diagnostic study only is requested, please check here. Reason _________________________________________
CPAP or BIPAP Titration/Retitration
Titration for patients with OSA documented by prior PSG.
*Diagnostic Sleep Study with Multiple Sleep Latency Test (MSLT) or Maintenance of Wakefulness Test (MWT). Diagnostic sleep study followed by a daytime nap test to diagnose narcolepsy or excessive daytime sleepiness.
*Both studies must be ordered by a neurologist, pulmonologist or sleep physician.
If PSG is abnormal, consultation with interpreting physician is requested for evaluation and management.
Please initial if this is desired _____________
Is patient going to be seen or has patient been seen in the past by one of the following:
*Please choose Sleep Reader/Consultant below
Albanese |
|
Patwa |
Bader |
|
Taylor |
|
||
Chervin |
|
Zaslow |
|
||
Gebhardt |
|
|
*No Preference - reading MD through rotation
MEDICAL HISTORY (history and physical examination is required). Please fax office notes/progress notes with request.
Weight _______________ lbs. |
Height _________________ |
BMI ____________ |
Neck Size _______________ in. |
Suspected Disorder(s)
Obstructive Sleep Apnea (OSA) Narcolepsy
Nocturnal Seizures/Parasomnias Insomnia
Restless legs syndrome (RLS) or periodic limb movements of sleep (PLMS)
Primary Symptoms
Snoring/gasping/choking Witnessed apnea Obese/large neck Daytime sleepiness Difficulty falling asleep Fragmented sleep
Frequent leg movements during sleep Preoperative assessment
Special Needs
Nocturnal O2 - Level: _________
Wheelchair Currently using PAP -
Pressure (cm): ____________
Other: _____________________
Medications/comments ________________________________________________________________________________________
___________________________________________________________________________________________________________
Please Circle
PMH: HTN DM COPD CAD CHF Depression Other
Physician's Signature _____________________________________________ Date/Time ________________________
WH1220 (01/10)