
ma 10 can be filled in online very easily. Simply use FormsPal PDF editor to do the job without delay. To retain our editor on the leading edge of efficiency, we strive to put into practice user-oriented capabilities and enhancements regularly. We're routinely looking for suggestions - join us in revampimg how we work with PDF docs. Starting is easy! Everything you should do is adhere to the next easy steps below:
Step 1: Press the "Get Form" button above. It will open our tool so you can begin filling in your form.
Step 2: When you start the PDF editor, you will find the form made ready to be filled out. Aside from filling in different blank fields, you can also perform other things with the form, particularly writing your own text, changing the original textual content, inserting graphics, putting your signature on the document, and a lot more.
Be attentive when completing this document. Ensure each and every blank is filled in properly.
1. Start filling out the ma 10 with a number of necessary blank fields. Gather all of the required information and make certain nothing is forgotten!
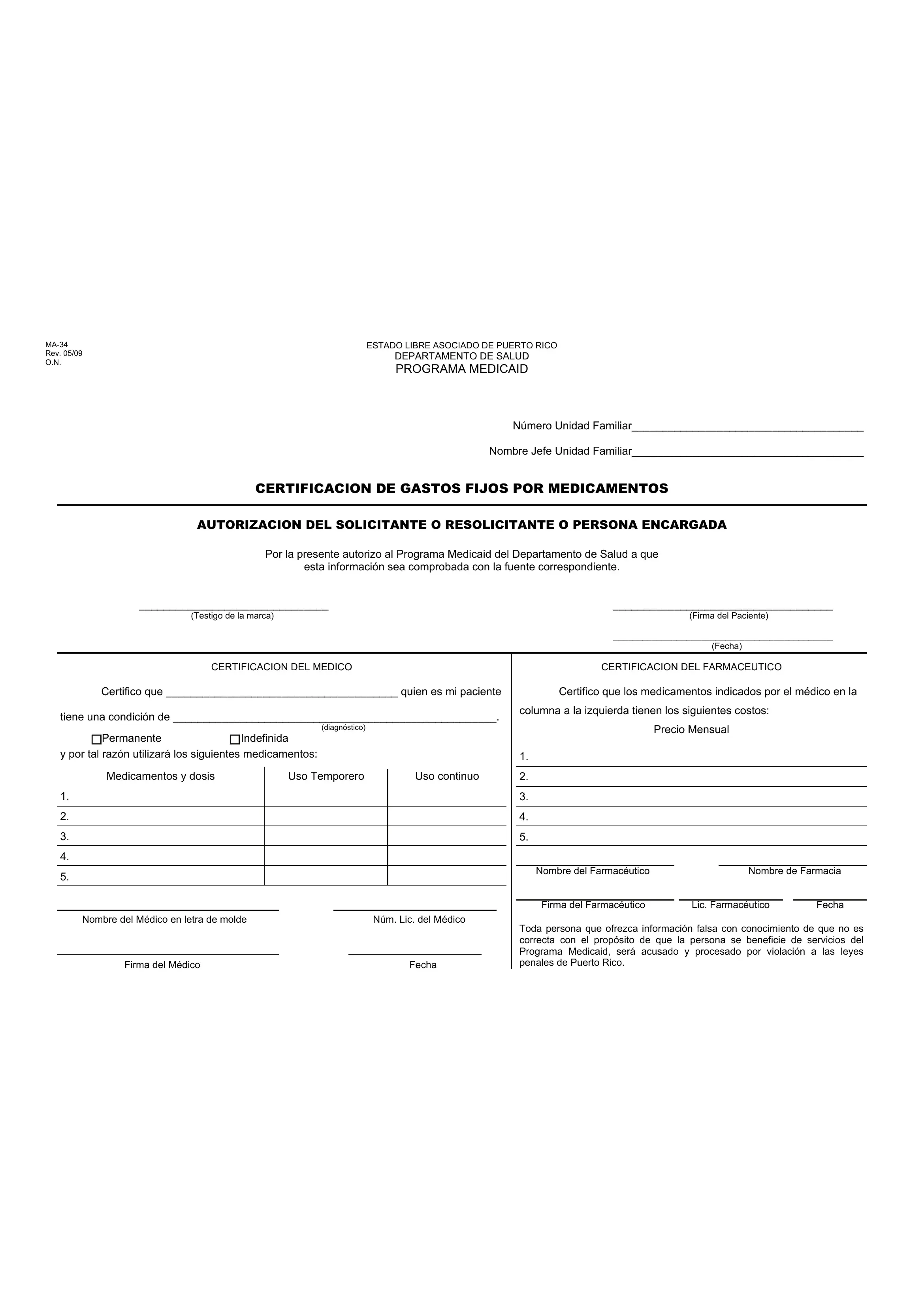
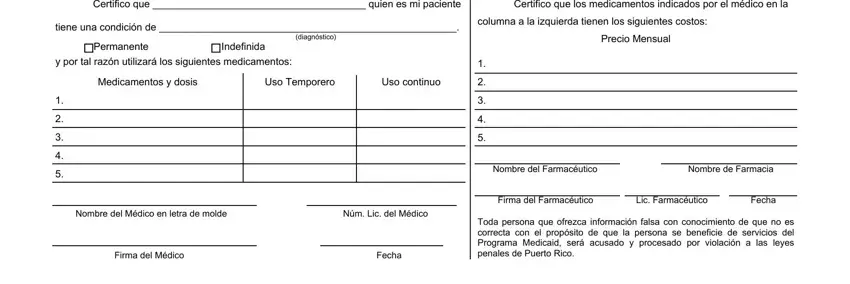
2. Once the last section is finished, you should add the required particulars in Certifico que quien es mi paciente, Certifico que los medicamentos, tiene una condición de, Permanente Indefinida, diagnóstico, y por tal razón utilizará los, Medicamentos y dosis, Uso Temporero, Uso continuo, Nombre del Médico en letra de, Firma del Médico, Fecha, columna a la izquierda tienen los, Precio Mensual, and Nombre del Farmacéutico Nombre de so that you can move forward to the next stage.
It is easy to make errors when completing your Fecha, for that reason be sure to look again before you finalize the form.
Step 3: Check that the information is correct and press "Done" to continue further. Download your ma 10 as soon as you sign up for a 7-day free trial. Conveniently access the document in your personal account, with any edits and adjustments being conveniently preserved! Whenever you work with FormsPal, you can certainly complete forms without the need to be concerned about personal information breaches or data entries being shared. Our protected system helps to ensure that your private details are stored safely.