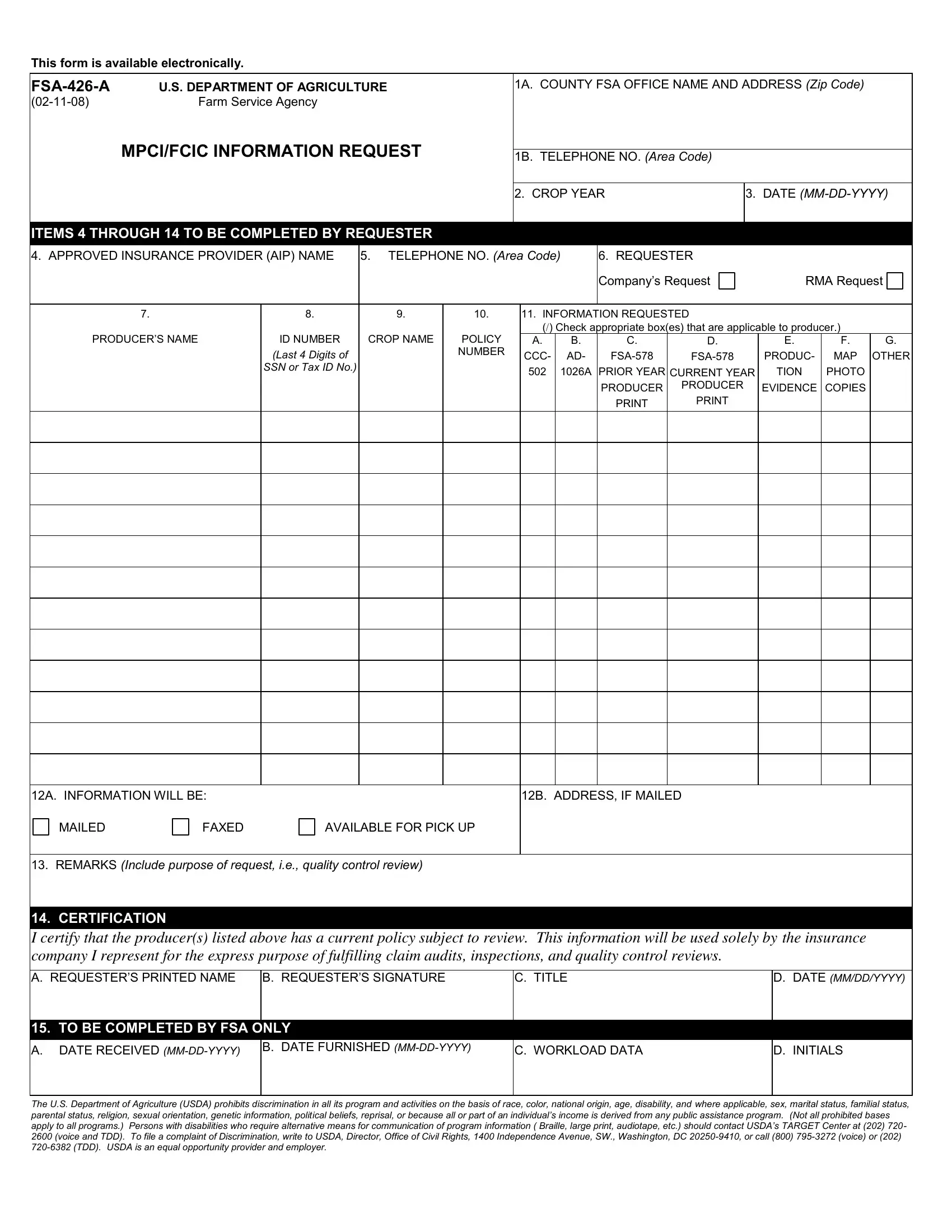
In the intricate process of managing agricultural operations under the purview of the U.S. Department of Agriculture (USDA), the FSA-426-A form plays a crucial role, facilitating a structured and efficient exchange of information between farmers, insurance providers, and the Farm Service Agency (FSA). Designed to streamline the request for vital information pertaining to Multi-Peril Crop Insurance (MPCI) and the Federal Crop Insurance Corporation (FCIC), this document ensures that agricultural professionals have a clear and accessible means to submit and receive data essential for the continuation of their work. Key elements include the provision of the county FSA office's contact details, specifics of the insurance policy in question, and a delineated set of requested information that covers a range of documentation from producer identification to evidence of production. Furthermore, by allowing for the specification of the mode of information delivery, whether by mail, fax, or pick-up, it underscores the USDA's commitment to accommodating diverse needs. Moreover, the form embodies the USDA's staunch stance against discrimination, asserting its role not only as a facilitator of agricultural endeavors but also as an advocate for equality and accessibility within its programs. Through its detailed certification section, it simultaneously reinforces the integrity and purposefulness of the information request, ensuring that data exchanged upholds the standards of quality control fundamental to the agricultural insurance sector.
| Question | Answer |
|---|---|
| Form Name | FSA-426-A Form |
| Form Length | 1 pages |
| Fillable? | Yes |
| Fillable fields | 140 |
| Avg. time to fill out | 28 min 19 sec |
| Other names | 426 mpci form, fsa form 426, mpci information request, fsa 426 request form |
This form is available electronically.
U.S. DEPARTMENT OF AGRICULTURE |
|
Farm Service Agency |
MPCI/FCIC INFORMATION REQUEST
1A. COUNTY FSA OFFICE NAME AND ADDRESS (Zip Code)
1B. TELEPHONE NO. (Area Code)
2. CROP YEAR |
3. DATE |
|
|
ITEMS 4 THROUGH 14 TO BE COMPLETED BY REQUESTER
4. APPROVED INSURANCE PROVIDER (AIP) NAME |
5. TELEPHONE NO. (Area Code) |
6. REQUESTER |
|
|
|
|||||
|
|
|
|
|
|
Company’s Request |
RMA Request |
|||
|
|
|
|
|
|
|
|
|
|
|
7. |
8. |
9. |
10. |
11. INFORMATION REQUESTED |
|
|
|
|||
PRODUCER’S NAME |
|
|
|
(/) Check appropriate box(es) that are applicable to producer.) |
|
|||||
ID NUMBER |
CROP NAME |
POLICY |
A. |
B. |
C. |
D. |
E. |
F. |
G. |
|
|
(Last 4 Digits of |
|
NUMBER |
CCC- |
AD- |
PRODUC- |
MAP |
OTHER |
||
|
|
|
||||||||
|
SSN or Tax ID No.) |
|
|
502 |
1026A |
PRIOR YEAR |
CURRENT YEAR |
TION |
PHOTO |
|
|
|
|
|
|
||||||
|
|
|
|
|
|
PRODUCER |
PRODUCER |
EVIDENCE |
COPIES |
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
12A. INFORMATION WILL BE: |
12B. ADDRESS, IF MAILED |
|
MAILED |
FAXED |
AVAILABLE FOR PICK UP |
13.REMARKS (Include purpose of request, i.e., quality control review)
14.CERTIFICATION
I certify that the producer(s) listed above has a current policy subject to review. This information will be used solely by the insurance company I represent for the express purpose of fulfilling claim audits, inspections, and quality control reviews.
A. REQUESTER’S PRINTED NAME
B. REQUESTER’S SIGNATURE
C. TITLE
D.DATE (MM/DD/YYYY)
15. TO BE COMPLETED BY FSA ONLY
A.DATE RECEIVED
B. DATE FURNISHED
C. WORKLOAD DATA
D. INITIALS
The U.S. Department of Agriculture (USDA) prohibits discrimination in all its program and activities on the basis of race, color, national origin, age, disability, and where applicable, sex, marital status, familial status, parental status, religion, sexual orientation, genetic information, political beliefs, reprisal, or because all or part of an individual’s income is derived from any public assistance program. (Not all prohibited bases apply to all programs.) Persons with disabilities who require alternative means for communication of program information ( Braille, large print, audiotape, etc.) should contact USDA’s TARGET Center at (202) 720-
2600 (voice and TDD). To file a complaint of Discrimination, write to USDA, Director, Office of Civil Rights, 1400 Independence Avenue, SW., Washington, DC