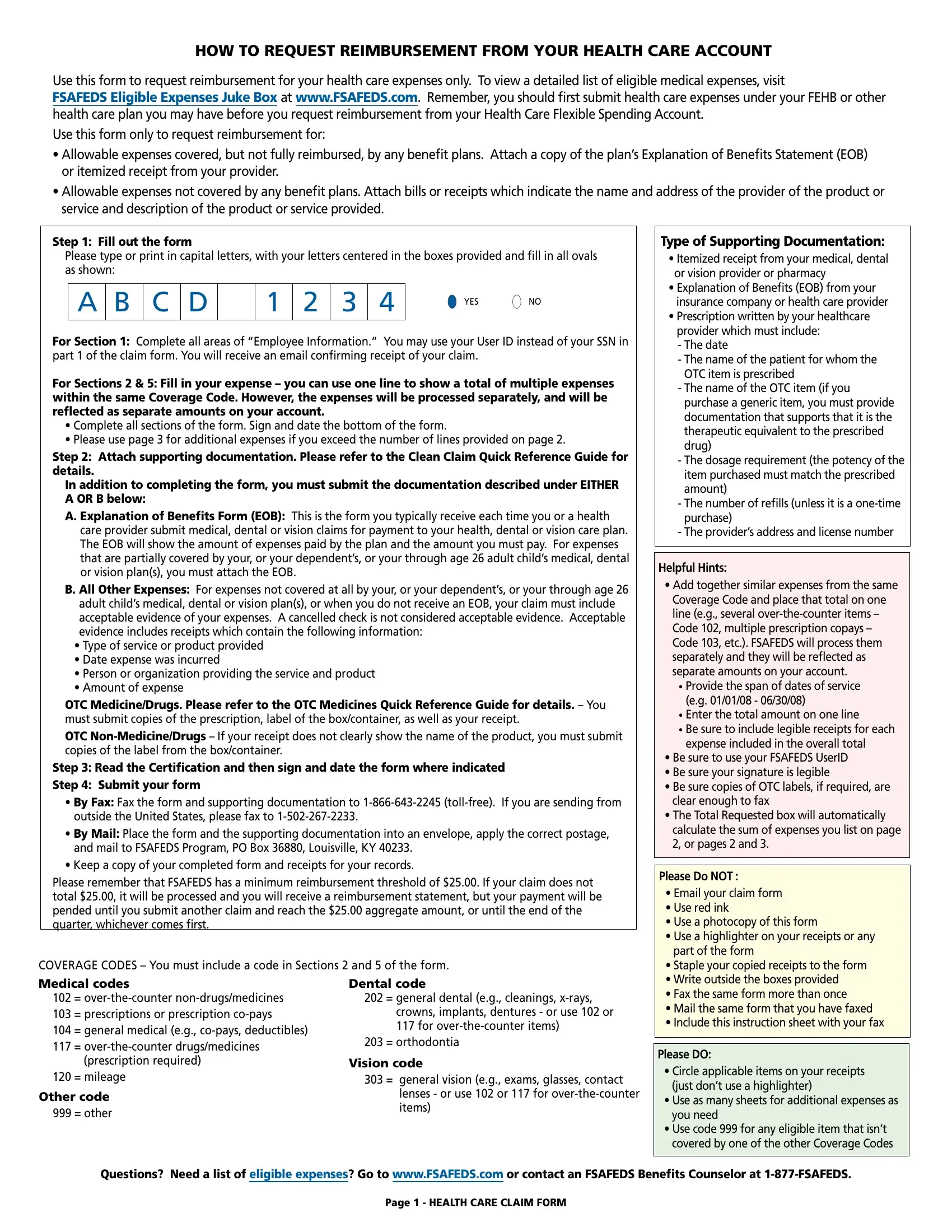
Navigating the realm of healthcare expenses can often feel overwhelming, but the FSAFEDS Claim Form serves as a beacon for federal employees seeking reimbursement for out-of-pocket healthcare costs. Tailored exclusively for use with Health Care Flexible Spending Accounts (HCFSAs), this form facilitates reimbursement for a broad array of medical expenses, from the partially covered by FEHB or other health plans to those not covered at all. A visit to the FSAFEDS website unlocks a comprehensive list of eligible expenses, ensuring users can confidently identify what qualifies for reimbursement. The process is straightforward: complete the form with pertinent details, attach the required documentation such as the Explanation of Benefits (EOB) or itemized receipts, and submit all through fax or mail. It's imperative to meticulously follow the instructions to avoid delays or denials, including the use of capital letters for filling out the form and the restriction against stapling documents. For expenses that extend beyond the provided space, additional pages are available, underscoring the form's flexibility to accommodate a range of healthcare financial needs. Engaging with the FSAFEDS Claim Form is more than an administrative task; it's a step toward maximizing the value of HCFSAs, ensuring federal employees and their families can lessen the financial burden of healthcare expenses.
| Question | Answer |
|---|---|
| Form Name | Fsafeds Claim Form |
| Form Length | 3 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 45 sec |
| Other names | fsafeds health claim, fsafeds health care claim form, fsafeds health online, fsafeds claim form |