The Family Support for Children with Disabilities (FSCD) application form serves as a vital first step for guardians seeking assistance through the FSCD program. This essential document collects detailed personal information under the Family Support for Children with Disabilities Act and Section 33(c) of the Freedom of Information and Protection of Privacy (FOIP) Act, ensuring that all data is handled with strict adherence to privacy laws. For families navigating the complexities of caring for children with disabilities, the form requests crucial information about the child, including diagnosis, citizenship status, and specific needs, as well as guardian details. It's important for applicants to provide accurate information and documentation, such as medical letters and proof of the child’s legal status in Canada, to facilitate the evaluation process. The application underscores the necessity of submitting a separate form for each child requiring support, emphasizing the program's attention to individual needs. Additionally, the form points guardians towards available resources for assistance and clarifies the use of personal information solely for the purpose of determining eligibility and providing tailored services to the family. Through this process, guardians are guided step by step, ensuring clarity and support as they seek to access the benefits of the FSCD program.
| Question | Answer |
|---|---|
| Form Name | FSCD Online Application Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | fscd online application, fscd application pdf, fscd application form pdf, fscd forms |
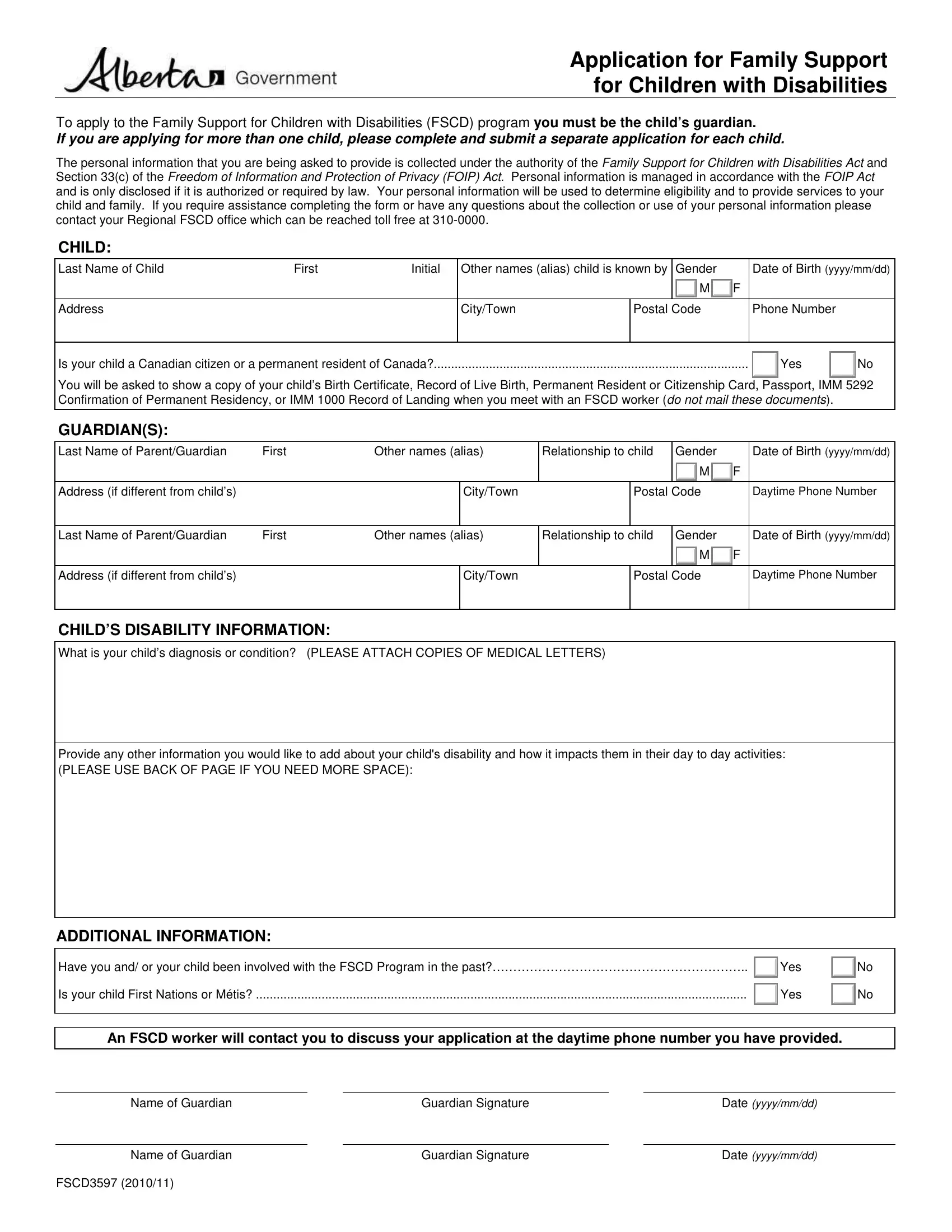
Application for Family Support for Children with Disabilities
To apply to the Family Support for Children with Disabilities (FSCD) program you must be the child’s guardian.
If you are applying for more than one child, please complete and submit a separate application for each child.
The personal information that you are being asked to provide is collected under the authority of the Family Support for Children with Disabilities Act and Section 33(c) of the Freedom of Information and Protection of Privacy (FOIP) Act. Personal information is managed in accordance with the FOIP Act and is only disclosed if it is authorized or required by law. Your personal information will be used to determine eligibility and to provide services to your child and family. If you require assistance completing the form or have any questions about the collection or use of your personal information please contact your Regional FSCD office which can be reached toll free at
CHILD:
Last Name of Child |
First |
Initial |
Other names (alias) child is known by |
Gender |
|
|
Date of Birth (yyyy/mm/dd) |
|||||||
|
|
|
|
|
|
|
M |
|
F |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Address |
|
|
City/Town |
Postal Code |
|
|
Phone Number |
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Is your child a Canadian citizen or a permanent resident of Canada? |
|
|
|
|
|
|
|
|
|
Yes |
|
No |
||
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
You will be asked to show a copy of your child’s Birth Certificate, Record of Live Birth, Permanent Resident or Citizenship Card, Passport, IMM 5292 Confirmation of Permanent Residency, or IMM 1000 Record of Landing when you meet with an FSCD worker (do not mail these documents).
GUARDIAN(S):
Last Name of Parent/Guardian |
First |
Other names (alias) |
|
Relationship to child |
|
Gender |
|
Date of Birth (yyyy/mm/dd) |
|||||
|
|
|
|
|
|
|
|
|
|
M |
|
F |
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Address (if different from child’s) |
|
|
City/Town |
|
|
Postal Code |
|
Daytime Phone Number |
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Last Name of Parent/Guardian |
First |
Other names (alias) |
|
Relationship to child |
|
Gender |
|
Date of Birth (yyyy/mm/dd) |
|||||
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
M |
|
F |
|
Address (if different from child’s) |
|
|
City/Town |
|
|
Postal Code |
|
Daytime Phone Number |
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
CHILD’S DISABILITY INFORMATION:
What is your child’s diagnosis or condition? (PLEASE ATTACH COPIES OF MEDICAL LETTERS)
Provide any other information you would like to add about your child's disability and how it impacts them in their day to day activities:
(PLEASE USE BACK OF PAGE IF YOU NEED MORE SPACE):
ADDITIONAL INFORMATION:
Have you and/ or your child been involved with the FSCD Program in the past?…………………………………………………….. |
|
Yes |
|
No |
|
|
|||
Is your child First Nations or Métis? |
|
Yes |
|
No |
|
|
|||
|
|
|||
|
|
|
|
|
|
|
|
|
|
An FSCD worker will contact you to discuss your application at the daytime phone number you have provided.
Name of Guardian |
|
Guardian Signature |
|
Date (yyyy/mm/dd) |
|
|
|
|
|
Name of Guardian |
|
Guardian Signature |
|
Date (yyyy/mm/dd) |
FSCD3597 (2010/11) |
|
|
|
|