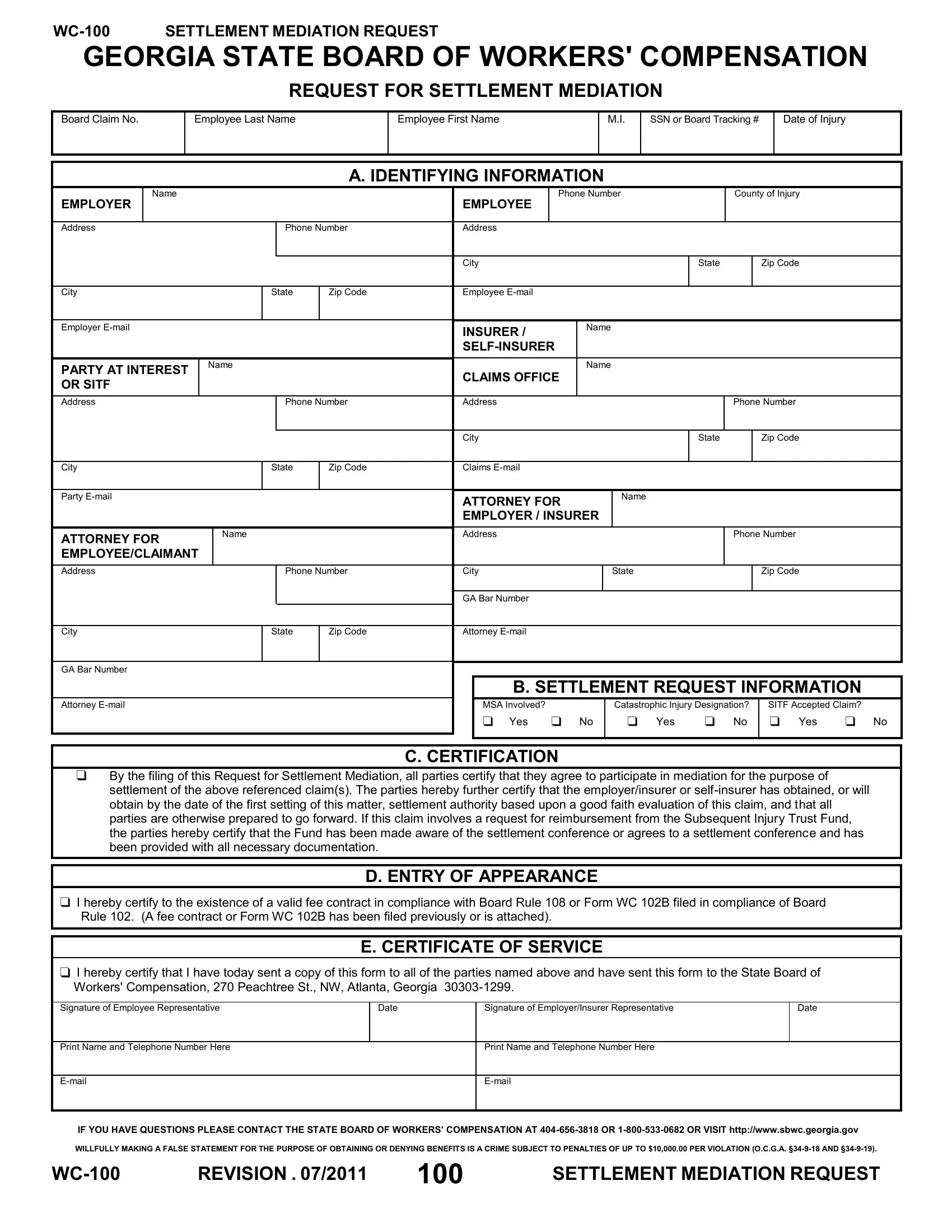
In the complex landscape of workers' compensation in Georgia, navigating the steps towards resolving disputes can be daunting for both employees and employers. One critical tool in this process is the WC-100 Settlement Mediation Request form, a document that plays a pivotal role in facilitating discussions aimed at settling claims out of the courtroom. This form is essential for initiating mediation under the auspices of the Georgia State Board of Workers' Compensation. It requires detailed information about the claim, including identification details of the employee, employer, and any insurance or self-insurer party involved. Moreover, it seeks specifics such as the date of injury, the presence of a catastrophic injury designation, and whether the claim involves the Subsequent Injury Trust Fund (SITF). The form's certification section underscores the commitment of all parties to engage in mediation with the intention of settling, ensuring they come prepared with the authority and readiness to negotiate in good faith. Importantly, this form must be properly filed with the certification of service, confirming its distribution to all relevant parties and the State Board of Workers' Compensation. In essence, the WC-100 form is not just a procedural step; it is a foundational move towards achieving resolution in what can often be a challenging and emotionally charged process.
| Question | Answer |
|---|---|
| Form Name | Georgia Form Wc 100 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | 102B, WC-100, NW, E-mail |
GEORGIA STATE BOARD OF WORKERS' COMPENSATION
REQUEST FOR SETTLEMENT MEDIATION
Board Claim No.
Employee Last Name
Employee First Name
M.I.
SSN or Board Tracking #
Date of Injury
A. IDENTIFYING INFORMATION
|
|
Name |
|
|
|
|
|
|
Phone Number |
|
County of Injury |
|||
|
EMPLOYER |
|
|
|
|
|
EMPLOYEE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Address |
|
|
Phone Number |
Address |
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
City |
|
|
State |
|
Zip Code |
||
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
City |
|
State |
Zip Code |
Employee |
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Employer |
|
|
|
|
INSURER / |
|
Name |
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PARTY AT INTEREST |
Name |
|
|
|
|
|
|
Name |
|
|
|
|
|
|
|
|
|
|
CLAIMS OFFICE |
|
|
|
|
|
||||
|
OR SITF |
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
Address |
|
|
Phone Number |
Address |
|
|
|
Phone Number |
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
City |
|
|
State |
|
Zip Code |
||
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
City |
|
State |
Zip Code |
Claims |
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Party
ATTORNEY FOR |
Name |
|
|
EMPLOYEE/CLAIMANT |
|
|
|
ATTORNEY FOR |
Name |
|
|
EMPLOYER / INSURER |
|
|
|
Address |
|
|
|
Phone Number
Address |
|
Phone Number |
City |
|
State |
|
|
Zip Code |
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
GA Bar Number |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
City |
State |
Zip Code |
Attorney |
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
GA Bar Number |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
B. SETTLEMENT REQUEST INFORMATION |
|
|||||
Attorney |
|
|
|
|
MSA Involved? |
|
Catastrophic Injury Designation? |
|
SITF Accepted Claim? |
|
|
|
|
|
|
|
Yes |
No |
Yes |
No |
|
Yes |
No |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
C. CERTIFICATION
By the filing of this Request for Settlement Mediation, all parties certify that they agree to participate in mediation for the purpose of settlement of the above referenced claim(s). The parties hereby further certify that the employer/insurer or
D. ENTRY OF APPEARANCE
I hereby certify to the existence of a valid fee contract in compliance with Board Rule 108 or Form WC 102B filed in compliance of Board Rule 102. (A fee contract or Form WC 102B has been filed previously or is attached).
E. CERTIFICATE OF SERVICE
I hereby certify that I have today sent a copy of this form to all of the parties named above and have sent this form to the State Board of Workers' Compensation, 270 Peachtree St., NW, Atlanta, Georgia
Signature of Employee Representative
Date
Signature of Employer/Insurer Representative
Date
Print Name and Telephone Number Here
Print Name and Telephone Number Here
IF YOU HAVE QUESTIONS PLEASE CONTACT THE STATE BOARD OF WORKERS’ COMPENSATION AT
WILLFULLY MAKING A FALSE STATEMENT FOR THE PURPOSE OF OBTAINING OR DENYING BENEFITS IS A CRIME SUBJECT TO PENALTIES OF UP TO $10,000.00 PER VIOLATION (O.C.G.A.
REVISION . 07/2011 |
100 |
SETTLEMENT MEDIATION REQUEST |