Georgia Form WC 100 is an important document that employees in the state of Georgia must complete to file for workers' compensation benefits. The form is used to provide information about the injury or illness and the employee's claim for benefits. Workers' compensation is a system of insurance that provides benefits to employees who are injured or become ill as a result of their job. If you have been injured or become ill as a result of your job, it is important to understand how workers' compensation can help you. The Georgia Department of Labor has more information on workers' compensation and how to file a claim.
| Question | Answer |
|---|---|
| Form Name | Georgia Form Wc 100 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | 102B, WC-100, NW, E-mail |
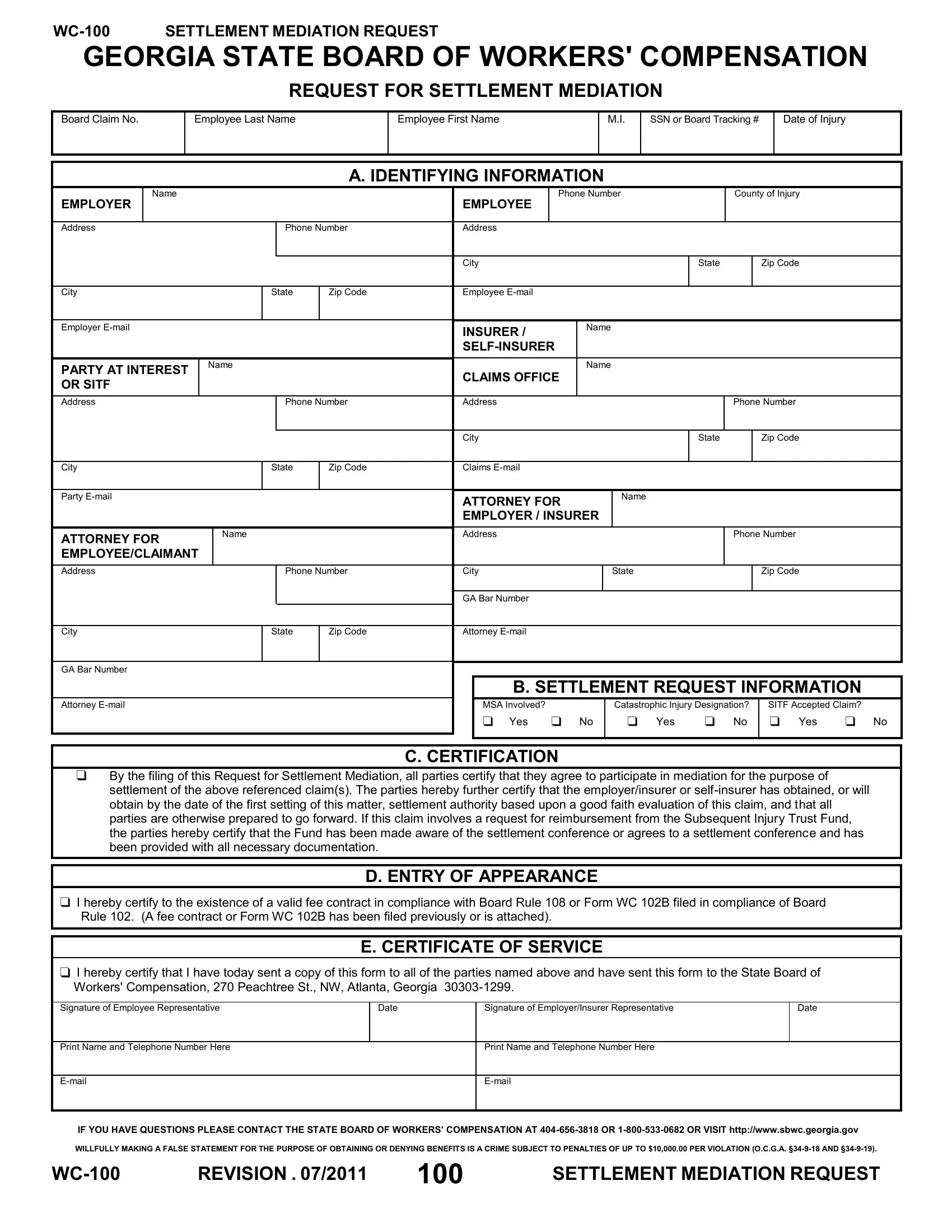
GEORGIA STATE BOARD OF WORKERS' COMPENSATION
REQUEST FOR SETTLEMENT MEDIATION
Board Claim No.
Employee Last Name
Employee First Name
M.I.
SSN or Board Tracking #
Date of Injury
A. IDENTIFYING INFORMATION
|
|
Name |
|
|
|
|
|
|
Phone Number |
|
County of Injury |
|||
|
EMPLOYER |
|
|
|
|
|
EMPLOYEE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Address |
|
|
Phone Number |
Address |
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
City |
|
|
State |
|
Zip Code |
||
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
City |
|
State |
Zip Code |
Employee |
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Employer |
|
|
|
|
INSURER / |
|
Name |
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PARTY AT INTEREST |
Name |
|
|
|
|
|
|
Name |
|
|
|
|
|
|
|
|
|
|
CLAIMS OFFICE |
|
|
|
|
|
||||
|
OR SITF |
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
Address |
|
|
Phone Number |
Address |
|
|
|
Phone Number |
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
City |
|
|
State |
|
Zip Code |
||
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
City |
|
State |
Zip Code |
Claims |
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Party
ATTORNEY FOR |
Name |
|
|
EMPLOYEE/CLAIMANT |
|
|
|
ATTORNEY FOR |
Name |
|
|
EMPLOYER / INSURER |
|
|
|
Address |
|
|
|
Phone Number
Address |
|
Phone Number |
City |
|
State |
|
|
Zip Code |
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
GA Bar Number |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
City |
State |
Zip Code |
Attorney |
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
GA Bar Number |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
B. SETTLEMENT REQUEST INFORMATION |
|
|||||
Attorney |
|
|
|
|
MSA Involved? |
|
Catastrophic Injury Designation? |
|
SITF Accepted Claim? |
|
|
|
|
|
|
|
Yes |
No |
Yes |
No |
|
Yes |
No |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
C. CERTIFICATION
By the filing of this Request for Settlement Mediation, all parties certify that they agree to participate in mediation for the purpose of settlement of the above referenced claim(s). The parties hereby further certify that the employer/insurer or
D. ENTRY OF APPEARANCE
I hereby certify to the existence of a valid fee contract in compliance with Board Rule 108 or Form WC 102B filed in compliance of Board Rule 102. (A fee contract or Form WC 102B has been filed previously or is attached).
E. CERTIFICATE OF SERVICE
I hereby certify that I have today sent a copy of this form to all of the parties named above and have sent this form to the State Board of Workers' Compensation, 270 Peachtree St., NW, Atlanta, Georgia
Signature of Employee Representative
Date
Signature of Employer/Insurer Representative
Date
Print Name and Telephone Number Here
Print Name and Telephone Number Here
IF YOU HAVE QUESTIONS PLEASE CONTACT THE STATE BOARD OF WORKERS’ COMPENSATION AT
WILLFULLY MAKING A FALSE STATEMENT FOR THE PURPOSE OF OBTAINING OR DENYING BENEFITS IS A CRIME SUBJECT TO PENALTIES OF UP TO $10,000.00 PER VIOLATION (O.C.G.A.
REVISION . 07/2011 |
100 |
SETTLEMENT MEDIATION REQUEST |