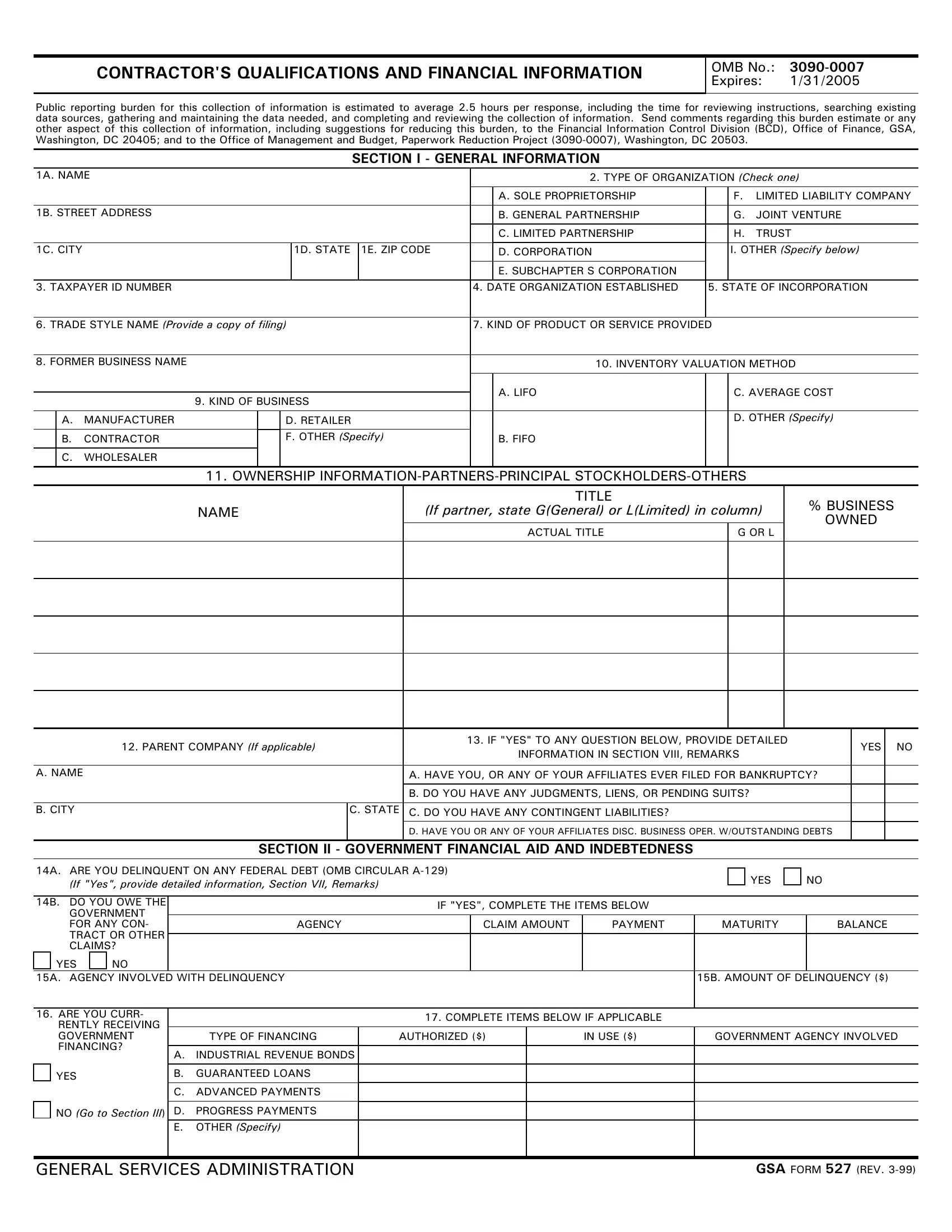
In the world of government contracting, transparency and financial stability are non-negotiable, which brings into focus the significance of the General Services Administration (GSA) Form 527, titled "Contractor's Qualifications and Financial Information." This form serves as a comprehensive tool, designed to collect a wide range of data from contractors aspiring to engage in business with government entities. Its content spans from general organizational details, such as the type of establishment and taxpayer identification number, to more specific financial data including inventory valuation methods, ownership details, and the fiscal health of the business. Additionally, it seeks information on any government financial assistance, income statements, and banking and finance details critical for assessing the financial stability and integrity of a contractor. Important too is the insight it offers into a contractor’s past performance and obligations, by probing for information on past bankruptcies, pending suits, or defaults on obligations. With its detailed sections and the requirement for prepared financial statements, the GSA Form 527 not only facilitates an understanding of a contractor's current financial standing but also acts as a vehicle for due diligence, aimed at preventing fraud and ensuring that only financially responsible entities engage in government contracts. Mandated every three years, this document underscores the government’s commitment to fiscal responsibility and operational integrity in its contractual engagements.
| Question | Answer |
|---|---|
| Form Name | Gsa Form 527 |
| Form Length | 6 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 1 min 30 sec |
| Other names | GSA_Form_527_fo r_SIN_246 54_Only gsa form 527 fillable |
CONTRACTOR'S QUALIFICATIONS AND FINANCIAL INFORMATION
OMB No.:
Expires: 1/31/2005
Public reporting burden for this collection of information is estimated to average 2.5 hours per response, including the time for reviewing instructions, searching existing data sources, gathering and maintaining the data needed, and completing and reviewing the collection of information. Send comments regarding this burden estimate or any other aspect of this collection of information, including suggestions for reducing this burden, to the Financial Information Control Division (BCD), Office of Finance, GSA, Washington, DC 20405; and to the Office of Management and Budget, Paperwork Reduction Project
SECTION I - GENERAL INFORMATION
1A. NAME |
|
|
|
|
|
|
2. TYPE OF ORGANIZATION (Check one) |
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
A. SOLE PROPRIETORSHIP |
|
F. |
LIMITED LIABILITY COMPANY |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
1B. STREET ADDRESS |
|
|
|
|
|
|
B. GENERAL PARTNERSHIP |
|
G. |
JOINT VENTURE |
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
C. LIMITED PARTNERSHIP |
|
H. |
TRUST |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
1C. CITY |
|
|
|
1D. STATE |
1E. ZIP CODE |
|
D. CORPORATION |
|
I. OTHER (Specify below) |
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
E. SUBCHAPTER S CORPORATION |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
3. |
TAXPAYER ID NUMBER |
|
|
|
|
|
4. |
DATE ORGANIZATION ESTABLISHED |
5. |
STATE OF INCORPORATION |
|||
|
|
|
|
|
|
|
|
||||||
6. |
TRADE STYLE NAME (Provide a copy of filing) |
7. KIND OF PRODUCT OR SERVICE PROVIDED |
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|||
8. |
FORMER BUSINESS NAME |
|
|
|
|
|
|
10. INVENTORY VALUATION METHOD |
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
A. LIFO |
|
C. AVERAGE COST |
|
|
|
|
|
9. KIND OF BUSINESS |
|
||||||||
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
||||
|
|
A. |
MANUFACTURER |
|
D. RETAILER |
|
|
|
D. OTHER (Specify) |
||||
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
B. |
CONTRACTOR |
|
F. OTHER (Specify) |
|
B. FIFO |
|
|
|
|||
C.WHOLESALER
11. OWNERSHIP
NAME
TITLE
(If partner, state G(General) or L(Limited) in column)
ACTUAL TITLE |
G OR L |
|
|
%BUSINESS OWNED
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
12. PARENT COMPANY (If applicable) |
|
13. IF "YES" TO ANY QUESTION BELOW, PROVIDE DETAILED |
YES |
NO |
||
|
INFORMATION IN SECTION VIII, REMARKS |
|||||
|
|
|
|
|||
|
|
|
|
|
|
|
A. NAME |
|
A. HAVE YOU, OR ANY OF YOUR AFFILIATES EVER FILED FOR BANKRUPTCY? |
|
|
||
|
|
|
|
|
|
|
|
|
B. DO YOU HAVE ANY JUDGMENTS, LIENS, OR PENDING SUITS? |
|
|
||
|
|
|
|
|
|
|
B. CITY |
C. STATE |
C. DO YOU HAVE ANY CONTINGENT LIABILITIES? |
|
|
||
|
|
|
|
|
|
|
|
|
D. HAVE YOU OR ANY OF YOUR AFFILIATES DISC. BUSINESS OPER. W/OUTSTANDING DEBTS |
|
|
||
SECTION II - GOVERNMENT FINANCIAL AID AND INDEBTEDNESS
14A. ARE YOU DELINQUENT ON ANY FEDERAL DEBT (OMB CIRCULAR
YES
NO
14B. DO YOU OWE THE |
|
|
IF "YES", COMPLETE THE ITEMS BELOW |
|
|
|||
GOVERNMENT |
|
|
|
|
||||
|
|
|
|
|
|
|
||
FOR ANY CON- |
|
AGENCY |
|
CLAIM AMOUNT |
PAYMENT |
MATURITY |
BALANCE |
|
TRACT OR OTHER |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
CLAIMS? |
|
|
|
|
|
|
|
|
YES |
NO |
|
|
|
|
|
|
|
15A. AGENCY INVOLVED WITH DELINQUENCY |
|
|
|
15B. AMOUNT OF DELINQUENCY ($) |
||||
|
|
|
|
|
|
|
|
|
16. ARE YOU CURR- |
|
|
17. COMPLETE ITEMS BELOW IF APPLICABLE |
|
|
|||
RENTLY RECEIVING |
|
|
|
|
||||
|
|
|
|
|
|
|
||
GOVERNMENT |
|
TYPE OF FINANCING |
AUTHORIZED ($) |
IN USE ($) |
GOVERNMENT AGENCY INVOLVED |
|||
FINANCING? |
|
|
|
|
|
|
|
|
A. |
INDUSTRIAL REVENUE BONDS |
|
|
|
|
|
||
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
YES |
|
B. |
GUARANTEED LOANS |
|
|
|
|
|
|
|
C. |
ADVANCED PAYMENTS |
|
|
|
|
|
NO (Go to Section III) D. PROGRESS PAYMENTS
E.OTHER (Specify)
GENERAL SERVICES ADMINISTRATION |
GSA FORM 527 (REV. |

SECTION III - FINANCIAL STATEMENTS
Prepared Financial Statements with notes may be provided in lieu of completing Section III
When financial statements are prepared or certified by independent accountants and transcribed |
18. ARE YOU THE INCUMBENT CONTRACTOR FOR THIS SOLICITATION |
||||||||||
|
|
|
|
|
|||||||
to this form, please furnish the name and address of accountant of accounting firm. |
|
|
YES |
|
|
|
NO |
||||
|
|
|
|
|
|
|
|
|
|
|
|
19A. NAME |
|
|
|
|
20. IF TRANSCRIBED STATEMENTS DIFFER FROM INDEPENDENT ACCOUNTANT'S, |
||||||
|
|
|
|
|
|||||||
|
|
|
|
|
|
PLEASE DESCRIBE ADJUSTMENT IN SECTION VII, REMARKS. ALL OF THE |
|||||
|
|
|
|
|
|
|
LISTED FIGURES ARE: |
||||
19B. STREET ADDRESS |
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
ACTUAL |
|
|
U.S. DOLLARS |
||
|
|
|
|
|
|
|
|
|
|
|
|
19C. CITY |
19D. STATE |
19E. ZIP CODE |
|
IN THOUSANDS |
|
|
FOREIGN CURRENCY (Specify) |
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
IN MILLIONS |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
21. BALANCE SHEET AS OF (Month, Day, Year) |
|
|
|
22. FISCAL |
YEAR |
ENDS (Month, Day, Year) |
|
|
|
23. PREPARED STMTS. |
|
|
|
|
|
|
|
|
|
|
|
|
ARE ATTACHED |
|
|
|
|
|
|
|
|||||
24. ASSETS |
|
|
25. LIABILITIES AND NET WORTH |
||||||||
|
|
|
|
|
|
|
|
|
|
||
A. Current Assets |
|
|
|
|
A. Current Liabilities |
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
Cash |
|
|
|
|
|
Accounts payable |
|
|
|
|
|
Short Term cash investments |
|
|
|
|
|
Notes payable (current) |
|
|
|
|
|
Accounts receivable, less allowance for |
|
|
Current portion of long term debt |
|
|||||||
doubtful accounts of $ |
|
|
|
|
|
Accrued expenses |
|
|
|
|
|
Inventories |
|
|
|
|
|
Accrued taxes on income/excess profits |
|
||||
Other current assets (Itemize below) |
|
|
Other current liabilities (Itemize) |
|
|||||||
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
Total Current Assets |
|
|
|
Total Current Liabilities |
|
||||||
B. Property, Plant and Equipment |
|
|
|
|
B. Other Liabilities |
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
Land |
|
|
|
|
|
Mortgages |
|
|
|
|
|
Buildings and equipment |
|
|
|
|
|
Bonds |
|
|
|
|
|
Leasehold improvements |
|
|
|
|
|
Deferred income taxes |
|
|
|
|
|
Less accumulated depreciation and |
|
|
|
|
|
Other long term debt |
|
|
|
|
|
amortization |
|
|
|
|
|
|
Total Other Liabilities |
|
|||
|
|
|
|
|
|
|
|
||||
Total Property, Plant and Equipment |
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
||||
C. Other Assets |
|
|
|
|
|
|
|
Total Liabilities |
|
||
|
|
|
|
|
|
|
|
|
|||
Investments in and advance to affiliated |
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
||||
company |
|
|
|
|
C. Minority Interest in Subsidiary |
|
|||||
Goodwill, less amortization |
|
|
|
|
D. Net Worth |
|
|
|
|
||
Due from officer, employee |
|
|
|
|
|
Preferred stock |
|
|
|
|
|
Other (Itemize) |
|
|
|
|
|
Common stock |
|
|
|
|
|
|
|
|
|
|
|
Additional |
|
|
|
|
|
|
|
|
|
|
|
Retained earnings/owner's equity |
|
||||
|
|
|
|
|
|
Less, Treasury stock |
|
|
|
|
|
Total Other Assets |
|
|
|
|
|
|
Total Net Worth |
|
|||
D. TOTAL ASSETS |
|
|
E. TOTAL LIABILITIES AND NET WORTH |
|
|||||||
|
|
|
|
|
|
|
|
||||
|
|
SECTION IV - INCOME STATEMENT |
|
|
|
|
|||||
26. FROM (Month, Day, Year)
27. TO (Month, Day, Year)
|
28. INCOME |
||
|
|
|
|
A. Net Sales |
|
Minority Interest in Earnings of |
|
Cost and Expenses |
|
Subsidiaries |
|
|
|
|
|
Cost of Goods Sold |
|
Total Costs and Expenses |
|
Depreciation and Amortization |
|
|
|
|
|
|
|
Selling, General, and Admin. Expenses |
|
Earnings Before Taxes |
|
Interest Expense |
|
Taxes on Income |
|
Other Expenses (Itemize) |
|
Income Before Extraordinary Items |
|
|
|
Extraordinary Gains (Losses) Net of Taxes |
|
|
|
NET INCOME (LOSS) |
|
|
|
GSA FORM 527 |
|
SECTION V - BANKING AND FINANCE COMPANY INFORMATION
(Please attach a separate sheet using this format for any additional banks.)
ITEM |
|
BANK 1 |
|
|
|
BANK 2 |
|
|
||
|
|
|
|
|
|
|
|
|
|
|
29.Name of Bank |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
30.Contact |
|
|
|
|
|
|
|
|
|
|
Person |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
31.Phone Number |
AREA CODE |
NUMBER |
|
EXT. |
AREA CODE |
NUMBER |
|
EXT. |
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
32.Fax Number |
AREA CODE |
NUMBER |
|
|
AREA CODE |
NUMBER |
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
STREET ADDRESS |
|
|
|
|
STREET ADDRESS |
|
|
|
|
33.Address |
|
|
|
|
|
|
|
|
|
|
CITY |
|
STATE |
ZIP CODE |
CITY |
|
STATE |
ZIP CODE |
|||
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
34.Amount |
|
|
|
|
|
|
|
|
|
|
Owing ($) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
35.Term Loans |
Yes |
|
No |
|
|
Yes |
|
No |
|
|
|
|
|
|
|
|
|
|
|
|
|
36.Line of Credit |
Yes |
|
No |
|
|
Yes |
|
No |
|
|
37.Maximum Amount Authorized ($)
38.Amount Outstanding ($)
39. Loans Secured by Company's Assets - Real and Personal Property
|
SECURED PARTY NAME |
|
|
|
CONTACT NAME |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
A. |
STREET ADDRESS |
|
CITY |
|
|
|
|
STATE |
ZIP CODE |
|
|
|
|
|
|
|
|
|
|
|
SECURING ASSETS |
|
|
|
|
|
MATURITY DATE |
MONTHLY |
PAYMENT ($) |
|
|
|
|
|
|
|
|
|
|
|
SECURED PARTY NAME |
|
|
|
CONTACT NAME |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
B. |
STREET ADDRESS |
|
CITY |
|
|
|
|
STATE |
ZIP CODE |
|
|
|
|
|
|
|
|
|
|
|
SECURING ASSETS |
|
|
|
|
|
MATURITY DATE |
MONTHLY |
PAYMENT ($) |
|
|
|
|
|
|
|
|
|
|
|
SECURED PARTY NAME |
|
|
|
CONTACT NAME |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
C. |
STREET ADDRESS |
|
CITY |
|
|
|
|
STATE |
ZIP CODE |
|
|
|
|
|
|
|
|
|
|
|
SECURING ASSETS |
|
|
|
|
|
MATURITY DATE |
MONTHLY |
PAYMENT ($) |
|
|
|
|
|
|
|
|
|
|
|
SECURED PARTY NAME |
|
|
|
CONTACT NAME |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
D. |
STREET ADDRESS |
|
CITY |
|
|
|
|
STATE |
ZIP CODE |
|
|
|
|
|
|
|
|
|
|
|
SECURING ASSETS |
|
|
|
|
|
MATURITY DATE |
MONTHLY |
PAYMENT ($) |
|
|
|
|
|
|
||||
40. |
ARE ANY OF THE ASSETS SHOWN ON THE BALANCE SHEET |
41A. |
IF CONTRACTOR IS A PARTNERSHIP OR SOLE PROPIERTORSHIP, ARE 41B. TOTAL |
||||||
|
PLEDGED OR MORTGAGED, EXCEPT AS STATED ABOVE? |
|
THE INDIVIDUAL LIABILITIES OF THE PROPIETOR(S) FOR FEDERAL |
LIABILITY ($) |
|||||
|
|
|
|
AND STATE INCOME AND/OR EXCESS PROFIT TAXES INCLUDED ON |
|
||||
|
|
|
|
THE BALANCE SHEET? |
|
|
|
|
|
|
NO |
YES (Explain in Section VII, Remarks) |
|
YES |
NO |
|
|
||
42. ARE YOU NOW IN OR PENDING DEFAULT ON ANY OBLIGATIONS, I.E., BANKS, FINANCIAL INSTITUTIONS, SUPPLIERS, OTHER?
NO
YES (Provide detailed information in Section VII, Remarks)
GSA FORM 527 (REV.
SECTION VI - PRINCIPAL MERCHANDISE OR RAW MATERIAL SUPPLIER INFORMATION
(Please attach separate sheet(s) using this format for additional suppliers.)
43. PAST DUE ACCOUNTS PAYABLE ($)
|
ITEM |
|
44. SUPPLIER 1 |
|
|
|
45. SUPPLIER 2 |
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
A. Name of Supplier |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
B. |
Contact Person |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
C. Telephone |
AREA CODE |
NUMBER |
|
EXT. |
AREA CODE |
NUMBER |
|
EXT. |
||||
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
D. Fax |
AREA CODE |
NUMBER |
|
|
AREA CODE |
NUMBER |
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
STREET ADDRESS |
|
|
|
|
STREET ADDRESS |
|
|
|
|
|
E. |
Address |
|
|
|
|
|
|
|
|
|
|
|
CITY |
|
STATE |
ZIP CODE |
CITY |
|
STATE |
ZIP CODE |
|||||
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
F. |
Amount Now |
|
|
|
|
|
|
|
|
|
|
|
|
Owing ($) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
G. |
High Credit ($) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
ITEM |
|
46. SUPPLIER 3 |
|
|
|
47. SUPPLIER 4 |
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
A. Name of Supplier |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
B. |
Contact Person |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
C. Telephone |
AREA CODE |
NUMBER |
|
EXT. |
AREA CODE |
NUMBER |
|
EXT. |
||||
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
D. Fax |
AREA CODE |
NUMBER |
|
|
AREA CODE |
NUMBER |
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
STREET ADDRESS |
|
|
|
|
STREET ADDRESS |
|
|
|
|
|
E. |
Address |
|
|
|
|
|
|
|
|
|
|
|
CITY |
|
STATE |
ZIP CODE |
CITY |
|
STATE |
ZIP CODE |
|||||
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
F. |
Amount Now |
|
|
|
|
|
|
|
|
|
|
|
|
Owing ($) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
G. High Credit ($) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
SECTION |
VII - CONSTRUCTION/SERVICE CONTRACTS INFORMATION (Public Buildings Service Contracts Only) |
|
|||||||||
|
|
|
|
CONTRACTS IN FORCE |
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
||
|
ITEM |
|
48. CONTRACT 1 |
|
|
|
49. CONTRACT 2 |
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
A. Location |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
B. Owner's Name |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
STREET ADDRESS |
|
|
|
|
STREET ADDRESS |
|
|
|
|
|
C. Address |
|
|
|
|
|
|
|
|
|
|
|
|
CITY |
|
STATE |
ZIP CODE |
CITY |
|
STATE |
ZIP CODE |
|||||
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
D.Type of Work
E.Contract Amt. ($)
F.% Completed
G.Est. Comp. Date
ITEM |
50. CONTRACT 3 |
51. CONTRACT 4 |
|
|
|
A.Location
B.Owner's Name
STREET ADDRESS |
STREET ADDRESS |
C. Address |
CITY |
STATE ZIP CODE |
CITY |
STATE ZIP CODE |
|
D.Type of Work
E.Contract Amt. ($)
F.% Completed
G.Est. Comp. Date
GSA FORM 527 (REV.
ITEM |
|
52. CONTRACT 5 |
|
53. CONTRACT 6 |
||||
|
|
|
|
|
|
|
|
|
A. Location |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
B. Owner's Name |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
STREET ADDRESS |
|
|
|
STREET ADDRESS |
|
|
|
C. Address |
|
|
|
|
|
|
|
|
CITY |
|
STATE |
ZIP CODE |
CITY |
|
STATE |
ZIP CODE |
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
D.Type of Work
E.Contract Amt. ($)
F.% Completed
G.Est. Comp. Date
ITEM |
54. CONTRACT 7 |
55. CONTRACT 8 |
|
|
|
A.Location
B.Owner's Name
STREET ADDRESS |
STREET ADDRESS |
C. Address |
CITY |
STATE ZIP CODE |
CITY |
STATE ZIP CODE |
|
D.Type of Work
E.Contract Amt. ($)
F.% Completed
G.Est. Comp. Date
|
LARGEST JOBS YOU HAVE COMPLETED IN THE LAST FIVE YEARS |
|
ITEM |
56. JOB 1 |
57. JOB 2 |
A.Location
B.Contact's Name
STREET ADDRESS |
STREET ADDRESS |
C. Address |
|
|
|
|
|
|
|
|
|
|
CITY |
|
STATE |
ZIP CODE |
CITY |
|
STATE |
ZIP CODE |
|||
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
D. Telephone |
AREA CODE |
NUMBER |
|
|
EXT. |
AREA CODE |
NUMBER |
|
|
EXT. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
E. Type of Work |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
F. Contract Amt. ($) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
G. Amount Sublet ($) |
|
|
|
|
|
|
|
|
|
|
ITEM |
|
58. JOB 3 |
|
|
|
59. JOB 4 |
|
|
||
A.Location
B.Contact's Name
STREET ADDRESS |
STREET ADDRESS |
C. Address |
|
|
|
|
|
|
|
|
|
|
CITY |
|
STATE |
ZIP CODE |
CITY |
|
STATE |
ZIP CODE |
|||
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
D. Telephone |
AREA CODE |
NUMBER |
|
|
EXT. |
AREA CODE |
NUMBER |
|
|
EXT. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
E. Type of Work |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
F. Contract Amt. ($) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
G. Amount Sublet ($) |
|
|
|
|
|
|
|
|
|
|
ITEM |
|
60. JOB 5 |
|
|
|
61. JOB 6 |
|
|
||
A.Location
B.Contact's Name
STREET ADDRESS |
STREET ADDRESS |
C. Address |
|
|
|
|
|
|
|
|
|
|
|
CITY |
|
STATE |
ZIP CODE |
CITY |
|
STATE |
ZIP CODE |
||||
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
D. Telephone |
AREA CODE |
NUMBER |
|
|
EXT. |
AREA CODE |
NUMBER |
|
|
EXT. |
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
E. |
Type of Work |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
F. |
Contract Amt. ($) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
G. |
Amount Sublet ($) |
|
|
|
|
|
|
|
|
|
|
GSA FORM 527 (REV.
|
LIST COMPANIES FROM WHOM YOU OBTAIN SURETY BONDS |
|
ITEM |
62. SURETY COMPANY 1 |
63. SURETY COMPANY 2 |
A.Company Name
B.Contact's Name
C. Telephone |
AREA CODE |
NUMBER |
|
|
EXT. |
AREA CODE |
NUMBER |
|
EXT. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
D. Fax |
AREA CODE |
NUMBER |
|
|
|
AREA CODE |
NUMBER |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
STREET ADDRESS |
|
|
|
|
STREET ADDRESS |
|
|
|
|
E. Address |
|
|
|
|
|
|
|
|
|
|
CITY |
|
STATE |
ZIP CODE |
CITY |
|
STATE |
ZIP CODE |
|||
|
|
|
||||||||
|
|
|
|
|
|
|
||||
64. PRESENT AMOUNT OF BONDING |
65. HAS YOUR |
APPLICATION |
FOR SURETY |
66. DURING THE PAST 2 YEARS, HAVE |
YOU BEEN |
CHARGED WITH A |
||||
COVERAGE ($) |
|
BOND EVER BEEN DECLINED (If Yes, please |
FAILURE TO MEET THE CLAIMS OF YOUR SUBCONTRACTORS OR |
|||||||
|
|
provide detailed information in Remarks) |
SUPPLIERS (If Yes, please provide detailed information in Remarks) |
|||||||
|
|
YES |
NO |
YES |
|
NO |
|
|
||
SECTION VIII - REMARKS
REMARKS (Cite those sections of the form relating to your remarks. If additional space is required, attach additional sheet(s).)
CERTIFICATION
For the purpose of establishing financial responsibility with, or procuring credit from the General Services Administration, we furnish the above as a true and correct statement of our financial condition and further certify that all other statements are true and correct. There has been no material change in the applicant's financial condition since the date of the above statement. We agree to notify you immediately in writing of any materially unfavorable change in our financial condition. In the absence of such notice or of a new and full financial statement, this is to be considered as a continuing statement.
NAME OF BUSINESS
BY (Signature of Authorized Official)
NAME OF AUTHORIZED OFFICIAL (Type or print) |
DATE |
|
|
TITLE OF AUTHORIZED OFFICIAL (Type or print) |
|
|
|
GSA FORM 527 (REV.