
Handling PDF forms online can be quite easy with this PDF editor. You can fill out gynecology intake form here effortlessly. Our editor is consistently developing to deliver the best user experience possible, and that is thanks to our commitment to continuous development and listening closely to customer feedback. In case you are seeking to get going, this is what it requires:
Step 1: Simply click the "Get Form Button" at the top of this webpage to launch our pdf file editing tool. Here you'll find all that is required to work with your document.
Step 2: The editor provides the opportunity to change your PDF in many different ways. Transform it by including your own text, correct original content, and put in a signature - all doable within a few minutes!
This document will need some specific information; in order to guarantee consistency, don't hesitate to take note of the tips directly below:
1. Firstly, once filling in the gynecology intake form, start in the section that has the subsequent blanks:
2. Once your current task is complete, take the next step – fill out all of these fields - DRUG NAMES, MEDICATIONS DOSAGE DRUG NAMES, GYN HISTORY, DOSAGE, Menstrual History What is the, and When was your last PAP smear Have with their corresponding information. Make sure to double check that everything has been entered correctly before continuing!
It's simple to make an error when filling out your DOSAGE, consequently you'll want to take a second look before you decide to send it in.
3. In this part, take a look at Have you ever tested positive for, PREGNANCY HISTORY, Number Number Number Total times, Full term deliveries Deliveries, and Cesarean sections Forceps or. Each of these must be taken care of with utmost accuracy.
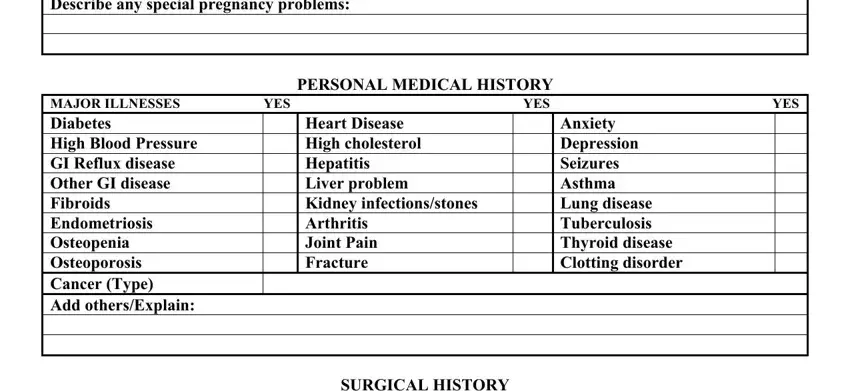
4. To move forward, this next stage involves completing several empty form fields. These include Number Number Number Total times, PERSONAL MEDICAL HISTORY, MAJOR ILLNESSES YES YES YES, Heart Disease High cholesterol, Anxiety Depression Seizures Asthma, and SURGICAL HISTORY, which you'll find essential to continuing with this PDF.
5. To finish your document, the particular subsection features several additional fields. Entering SURGERY YEAR SURGERY YEAR will certainly conclude everything and you will be done in the blink of an eye!
Step 3: Right after looking through your fields and details, click "Done" and you're good to go! Join us right now and instantly obtain gynecology intake form, ready for downloading. Each and every change made is handily saved , helping you to modify the file later on anytime. FormsPal is dedicated to the confidentiality of our users; we always make sure that all information used in our tool remains secure.