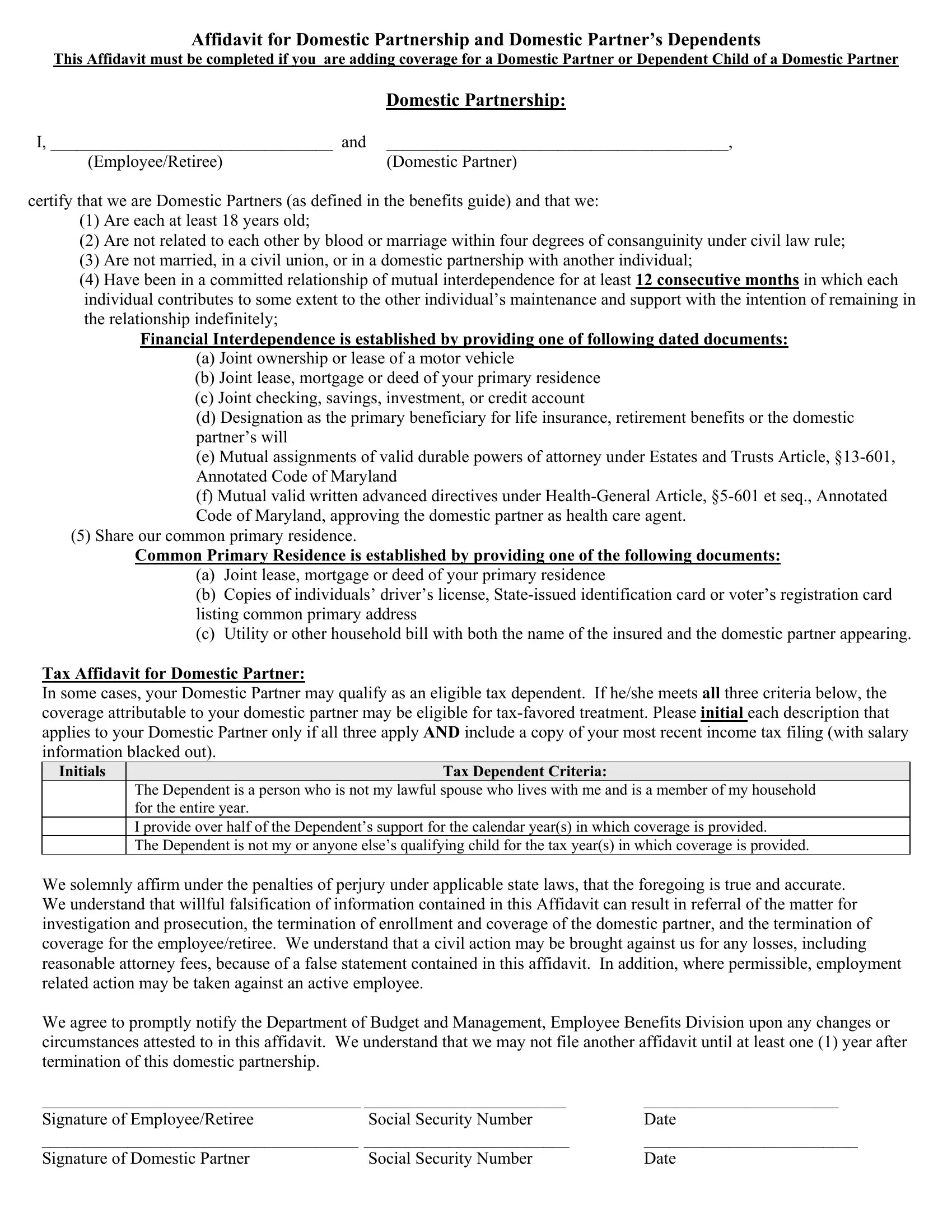
In Maryland, the process of recognizing a domestic partnership and extending benefits to a domestic partner and their dependents involves a detailed legal procedure, as outlined in the Maryland Domestic Partnership form. This form, crucial for domestic partners seeking to avail themselves of shared benefits, requires comprehensive information and affirmations from both parties involved. Central to this form is the Affidavit for Domestic Partnership and Domestic Partner’s Dependents, which mandates that both partners declare their commitment to a mutually supportive relationship that is intended to be indefinite. Partners must confirm that they are over the age of 18, not related by blood or marriage within a prohibited degree, not currently married or in a domestic partnership with someone else, and have lived together in a relationship of mutual interdependence for at least 12 consecutive months. Documentary evidence, such as joint ownership or lease documents, shared financial accounts, and mutual designations in legal documents like wills or health care directives, is required to demonstrate financial interdependence and a common primary residence. Additionally, the form inquires about the eligibility of the domestic partner for tax-favored treatment based on dependency criteria, further emphasizing the form’s role in aligning domestic partnerships with recognized legal and financial frameworks. This meticulously designed affidavit ensures that domestic partners and their dependents can achieve a semblance of the legal recognition and benefits traditionally reserved for married couples, upon successful submission and approval of the required documentation.
| Question | Answer |
|---|---|
| Form Name | Maryland Domestic Partnership Form |
| Form Length | 3 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 45 sec |
| Other names | maryland domestic partnership application, baltimore county domestic partnership, maryland affidavit partnership, maryland affidavit partnership domestic |