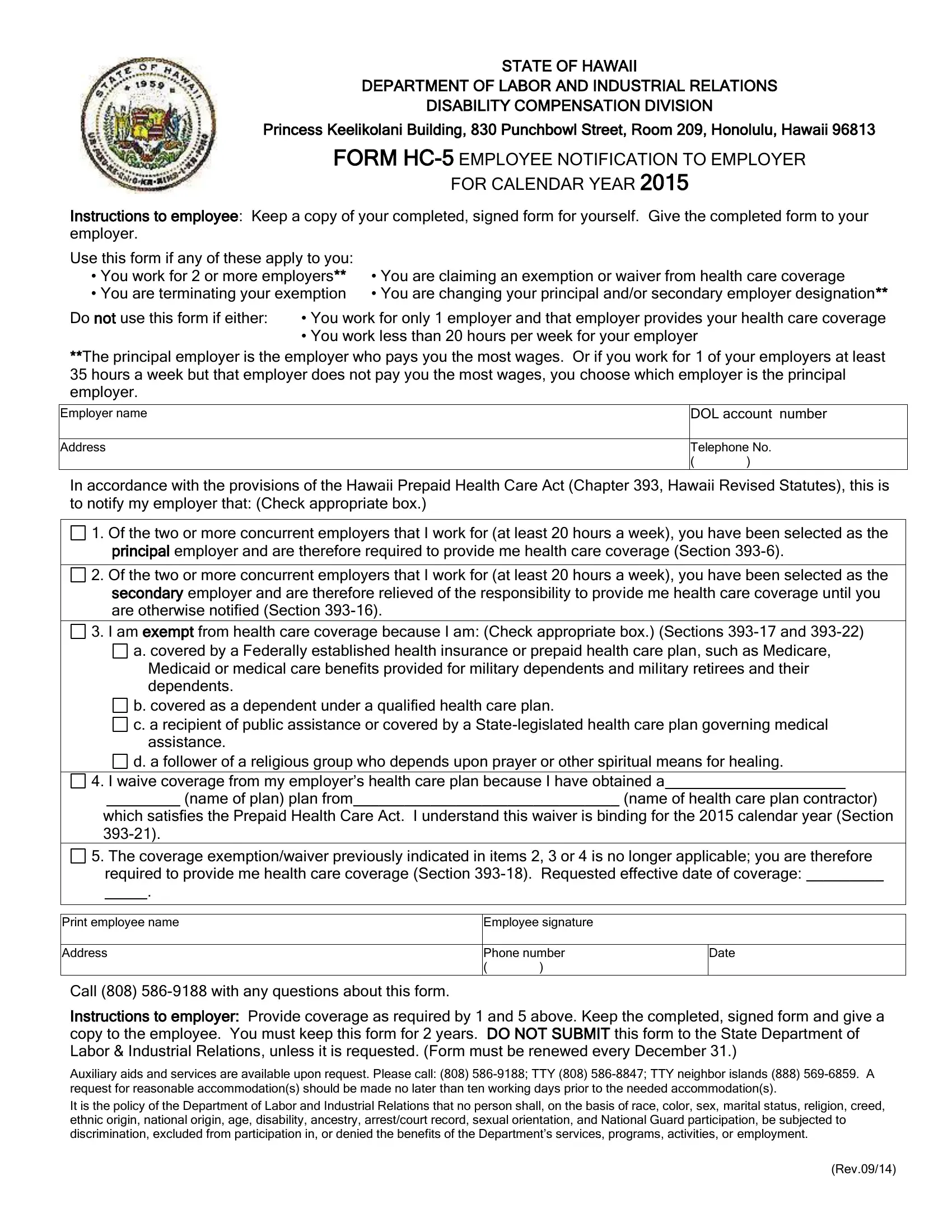
In the captivating realm of employee rights and employer responsibilities in Hawaii, the HC-5 form emerges as a pivotal document, bridging the gap between regulatory requirements and individual employment circumstances. Crafted by the State of Hawaii Department of Labor and Industrial Relations, the Disability Compensation Division, this essential form finds its purpose nestled within the ambit of the Hawaii Prepaid Health Care Act. Situated at the heart of Honolulu within the Princess Keelikolani Building, the division oversees the execution of HC-5, providing a structured avenue for employees to communicate specific health coverage statuses to their employers for the calendar year. The form primarily caters to employees working for multiple employers, those seeking exemptions or waivers from health care coverage, or individuals marking changes in their coverage preferences or employment scenarios. It precisely outlines various scenarios under which an employee might opt-out of employer-provided health care, adjust provider designations amongst multiple employers, or declare coverage through alternative plans satisfying state health care requirements. Central to maintaining compliance with Chapter 393 of the Hawaii Revised Statutes, it underscores the commitment of both the state and its workforce to uphold superior standards of health care accessibility and personal choice. Moreover, the underlying ethos of the form encapsulates a broader commitment to fairness and inclusivity, as echoed in the Department's non-discrimination policy, ensuring every employee's right to health care benefits is recognized and respected, devoid of undue burden or prejudice.
| Question | Answer |
|---|---|
| Form Name | Hawaii Form HC-5 |
| Form Length | 1 pages |
| Fillable? | Yes |
| Fillable fields | 12 |
| Avg. time to fill out | 2 min 43 sec |
| Other names | hc 15 form, hawaii notification, hc 5 form, what is hc 5 form |
STATE OF HAWAII
DEPARTMENT OF LABOR AND INDUSTRIAL RELATIONS
DISABILITY COMPENSATION DIVISION
Princess Keelikolani Building, 830 Punchbowl Street, Room 209, Honolulu, Hawaii 96813
FORM
FOR CALENDAR YEAR 2015
Instructions to employee: Keep a copy of your completed, signed form for yourself. Give the completed form to your employer.
Use this form if any of these apply to you:
•You work for 2 or more employers** • You are claiming an exemption or waiver from health care coverage
•You are terminating your exemption • You are changing your principal and/or secondary employer designation**
Do not use this form if either: • You work for only 1 employer and that employer provides your health care coverage
•You work less than 20 hours per week for your employer
**The principal employer is the employer who pays you the most wages. Or if you work for 1 of your employers at least 35 hours a week but that employer does not pay you the most wages, you choose which employer is the principal employer.
Employer name
Address
DOL account number
__ __ __ __ __ __ __ __ __ __
Telephone No.
()
In accordance with the provisions of the Hawaii Prepaid Health Care Act (Chapter 393, Hawaii Revised Statutes), this is to notify my employer that: (Check appropriate box.)
1. Of the two or more concurrent employers that I work for (at least 20 hours a week), you have been selected as the principal employer and are therefore required to provide me health care coverage (Section
2. Of the two or more concurrent employers that I work for (at least 20 hours a week), you have been selected as the secondary employer and are therefore relieved of the responsibility to provide me health care coverage until you are otherwise notified (Section
3. I am exempt from health care coverage because I am: (Check appropriate box.) (Sections
a. covered by a Federally established health insurance or prepaid health care plan, such as Medicare, Medicaid or medical care benefits provided for military dependents and military retirees and their dependents.
b. covered as a dependent under a qualified health care plan.
c. a recipient of public assistance or covered by a
d. a follower of a religious group who depends upon prayer or other spiritual means for healing.
4. I waive coverage from my employer’s health care plan because I have obtained a_____________________
_(name of plan) plan from_______________________________ (name of health care plan contractor) which satisfies the Prepaid Health Care Act. I understand this waiver is binding for the 2015 calendar year (Section
5. The coverage exemption/waiver previously indicated in items 2, 3 or 4 is no longer applicable; you are therefore required to provide me health care coverage (Section
_ ___.
Print employee name |
Employee signature |
|
|
|
|
|
|
Address |
Phone number |
Date |
|
|
( |
) |
|
Call (808)
Instructions to employer: Provide coverage as required by 1 and 5 above. Keep the completed, signed form and give a copy to the employee. You must keep this form for 2 years. DO NOT SUBMIT this form to the State Department of Labor & Industrial Relations, unless it is requested. (Form must be renewed every December 31.)
Auxiliary aids and services are available upon request. Please call: (808)
It is the policy of the Department of Labor and Industrial Relations that no person shall, on the basis of race, color, sex, marital status, religion, creed,
ethnic origin, national origin, age, disability, ancestry, arrest/court record, sexual orientation, and National Guard participation, be subjected to discrimination, excluded from participation in, or denied the benefits of the Department’s services, programs, activities, or employment.
(Rev.09/14)