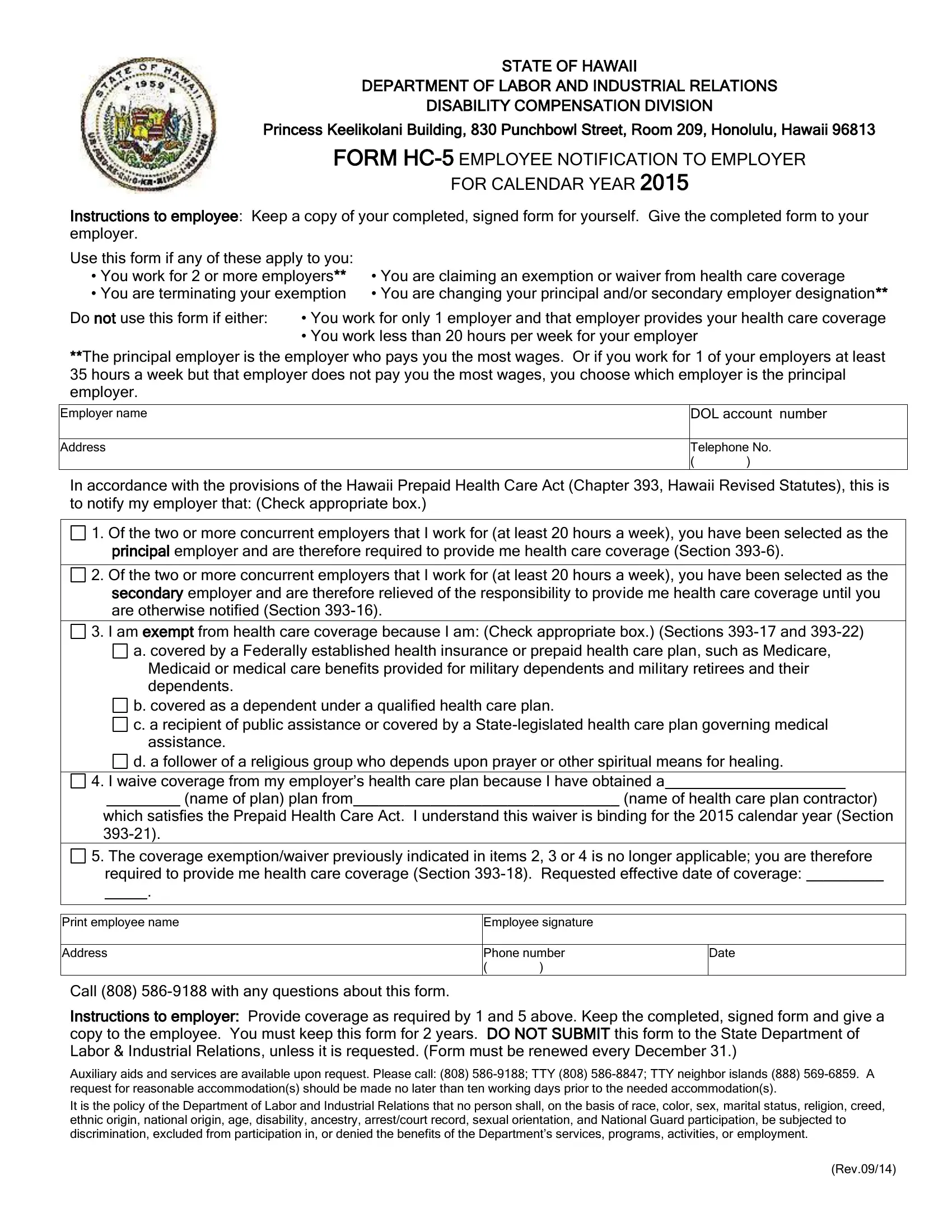
In the captivating realm of employee rights and employer responsibilities in Hawaii, the HC-5 form emerges as a pivotal document, bridging the gap between regulatory requirements and individual employment circumstances. Crafted by the State of Hawaii Department of Labor and Industrial Relations, the Disability Compensation Division, this essential form finds its purpose nestled within the ambit of the Hawaii Prepaid Health Care Act. Situated at the heart of Honolulu within the Princess Keelikolani Building, the division oversees the execution of HC-5, providing a structured avenue for employees to communicate specific health coverage statuses to their employers for the calendar year. The form primarily caters to employees working for multiple employers, those seeking exemptions or waivers from health care coverage, or individuals marking changes in their coverage preferences or employment scenarios. It precisely outlines various scenarios under which an employee might opt-out of employer-provided health care, adjust provider designations amongst multiple employers, or declare coverage through alternative plans satisfying state health care requirements. Central to maintaining compliance with Chapter 393 of the Hawaii Revised Statutes, it underscores the commitment of both the state and its workforce to uphold superior standards of health care accessibility and personal choice. Moreover, the underlying ethos of the form encapsulates a broader commitment to fairness and inclusivity, as echoed in the Department's non-discrimination policy, ensuring every employee's right to health care benefits is recognized and respected, devoid of undue burden or prejudice.
| Question | Answer |
|---|---|
| Form Name | Hawaii Form HC-5 |
| Form Length | 1 pages |
| Fillable? | Yes |
| Fillable fields | 12 |
| Avg. time to fill out | 2 min 43 sec |
| Other names | hc 15 form, hawaii notification, hc 5 form, what is hc 5 form |