
Working with PDF documents online can be easy with this PDF editor. Anyone can fill out kokua mau polst here effortlessly. Our tool is constantly developing to give the very best user experience possible, and that is because of our commitment to continuous development and listening closely to user opinions. By taking a couple of basic steps, you may begin your PDF editing:
Step 1: First of all, open the editor by clicking the "Get Form Button" in the top section of this site.
Step 2: With our state-of-the-art PDF file editor, you're able to accomplish more than simply fill in forms. Edit away and make your documents appear perfect with customized textual content added in, or fine-tune the original input to perfection - all supported by an ability to incorporate your personal pictures and sign the document off.
This PDF will require specific information to be filled out, thus be sure you take your time to enter exactly what is required:
1. When filling out the kokua mau polst, ensure to include all of the essential fields in its corresponding area. This will help facilitate the process, enabling your information to be handled fast and accurately.
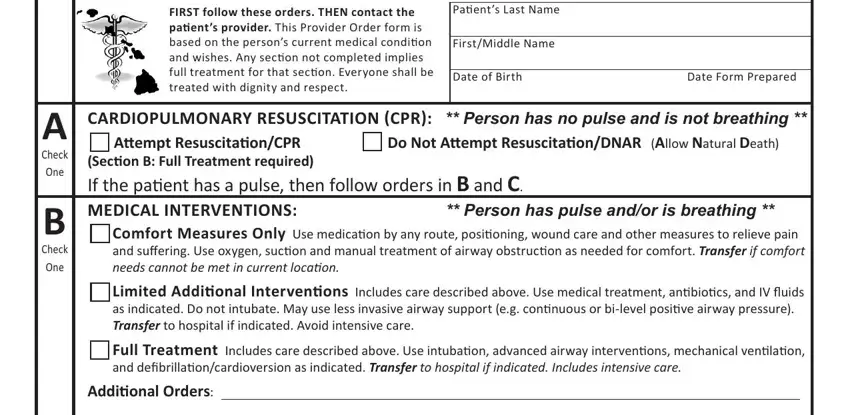
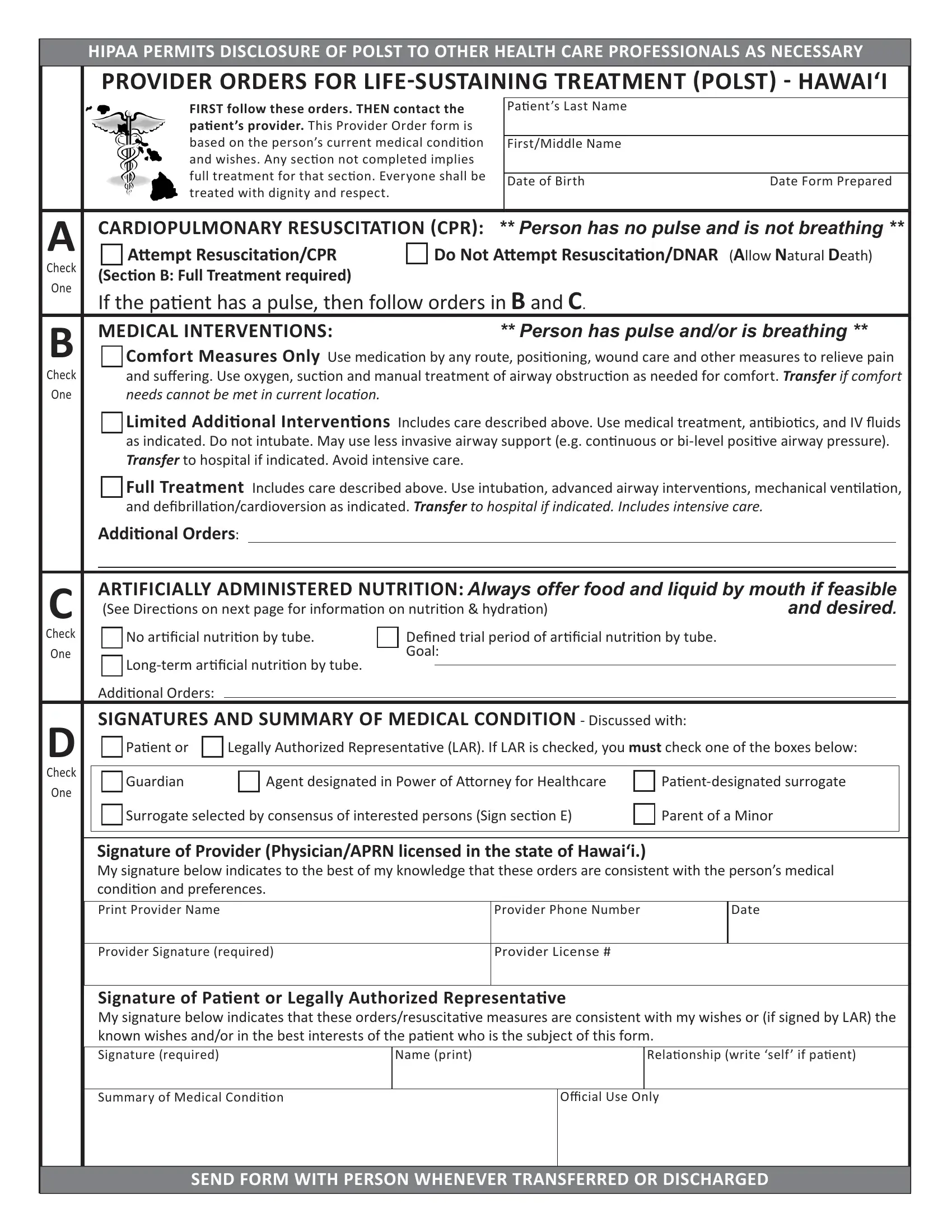
2. Once your current task is complete, take the next step – fill out all of these fields - Check One, Check One, ARTIFICIALLY ADMINISTERED, No arificial nutriion by tube, Goal, Addiional Orders SIGNATURES AND, Paient or, Legally Authorized Representaive, Guardian, Agent designated in Power of, Paientdesignated surrogate, Surrogate selected by consensus of, Parent of a Minor, Signature of Provider, and Provider Phone Number with their corresponding information. Make sure to double check that everything has been entered correctly before continuing!
As to No arificial nutriion by tube and ARTIFICIALLY ADMINISTERED, be certain you double-check them in this section. Those two could be the most significant ones in the page.
3. The next stage is generally straightforward - complete every one of the empty fields in Signature of Paient or Legally, Relaionship write self if paient, Name print, Summary of Medical Condiion, Official Use Only, and SEND FORM WITH PERSON WHENEVER in order to finish this process.

4. It's time to proceed to this next section! In this case you'll have these HIPAA PERMITS DISCLOSURE OF POLST, Paient Name last first middle, Date of Birth, Gender, M F, Patients Preferred Emergency, Name, Address, Phone Number, Health Care Professional Preparing, Preparer Title, Phone Number, Date Form Prepared, SURROGATE SELECTED BY CONSENSUS OF, and Signature required empty form fields to fill in.
Step 3: When you've reread the information in the blanks, press "Done" to complete your FormsPal process. Go for a 7-day free trial account with us and gain instant access to kokua mau polst - downloadable, emailable, and editable from your FormsPal cabinet. FormsPal is devoted to the confidentiality of all our users; we ensure that all personal data entered into our editor continues to be secure.