
With the help of the online editor for PDFs by FormsPal, you'll be able to fill in or modify icf form 02 02 97 here and now. To keep our editor on the leading edge of efficiency, we strive to integrate user-driven capabilities and enhancements on a regular basis. We're routinely looking for feedback - assist us with reshaping the way you work with PDF docs. To begin your journey, consider these easy steps:
Step 1: First of all, open the pdf tool by pressing the "Get Form Button" in the top section of this site.
Step 2: With this online PDF editor, you'll be able to do more than merely fill in forms. Try all the features and make your docs seem professional with customized text added in, or adjust the original content to perfection - all that backed up by an ability to incorporate any images and sign the PDF off.
With regards to the blanks of this specific PDF, here's what you need to know:
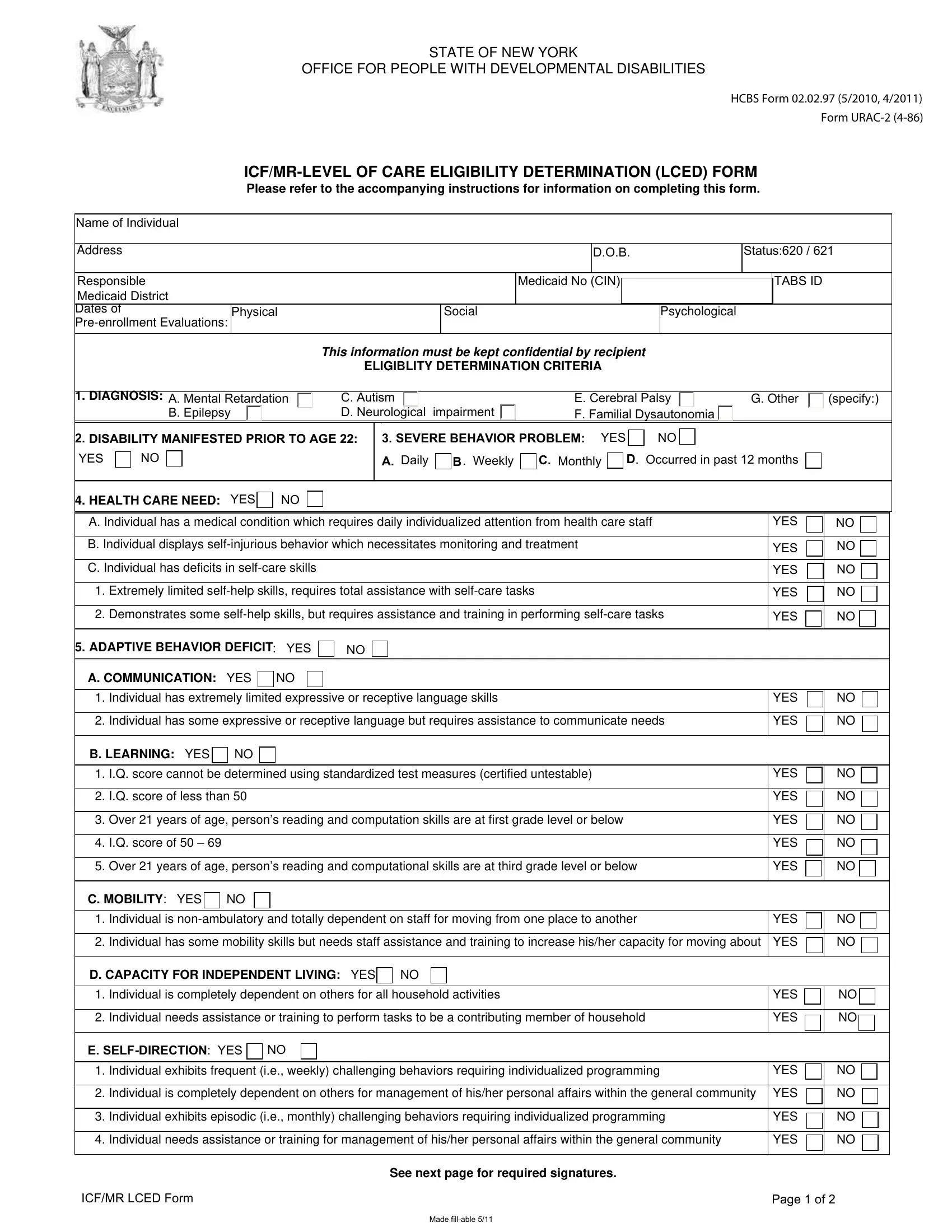
1. The icf form 02 02 97 needs particular details to be entered. Ensure the next fields are filled out:
2. Soon after completing the last section, go on to the next part and enter all required particulars in all these fields - Demonstrates some selfhelp skills, ADAPTIVE BEHAVIOR DEFICIT YES, A COMMUNICATION YES, Individual has extremely limited, Individual has some expressive or, B LEARNING YES, IQ score cannot be determined, IQ score of less than, Over years of age persons, IQ score of, Over years of age persons, C MOBILITY YES, Individual is nonambulatory and, YES, and YES.
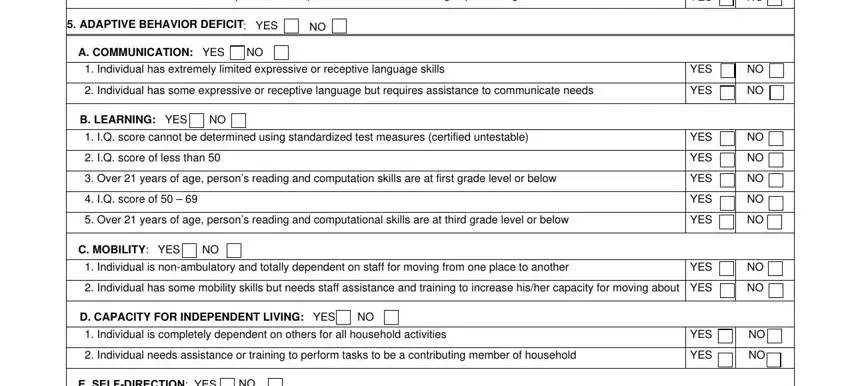
3. Your next part is usually straightforward - fill in every one of the fields in E SELFDIRECTION YES, Individual exhibits frequent ie, YES, Individual is completely, Individual exhibits episodic ie, Individual needs assistance or, YES, YES, ICFMR LCED Form, Page of, Made fillable, and See next page for required to conclude this part.

As for YES and Individual is completely, be sure that you take another look in this section. Those two are definitely the most significant fields in this form.
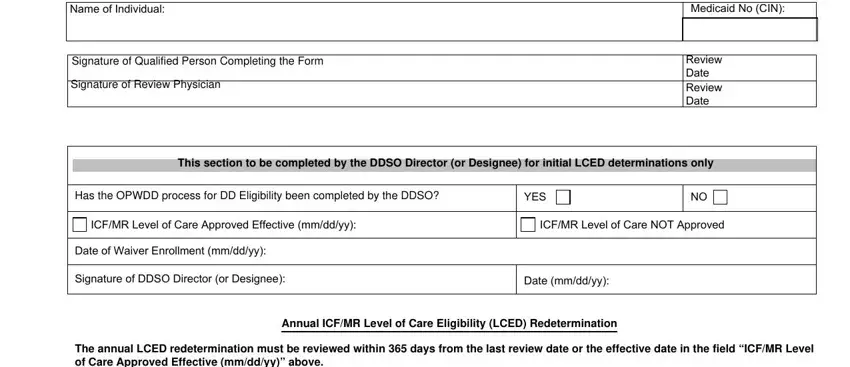
4. All set to start working on this next portion! Here you've got all these Name of Individual, Medicaid No CIN, Signature of Qualified Person, Signature of Review Physician, Review Date Review Date, This section to be completed by, Has the OPWDD process for DD, YES, ICFMR Level of Care Approved, ICFMR Level of Care NOT Approved, Date of Waiver Enrollment mmddyy, Signature of DDSO Director or, Date mmddyy, Annual ICFMR Level of Care, and The annual LCED redetermination blanks to fill in.
5. This form should be wrapped up with this particular segment. Here you can see an extensive list of form fields that require appropriate information for your document submission to be faultless: Signature and Title of Qualified, Review Date, Note If an individual no longer, ICFMR LCED Form, and Page of.
Step 3: Soon after going through the form fields you've filled in, click "Done" and you are done and dusted! Sign up with us today and easily use icf form 02 02 97, available for downloading. Every single edit you make is handily saved , allowing you to modify the document at a later time when necessary. We don't share or sell the information you use while dealing with forms at our website.