|
|
|
|
|
|
|
|
(Patient Identification) |
|
|
|
|
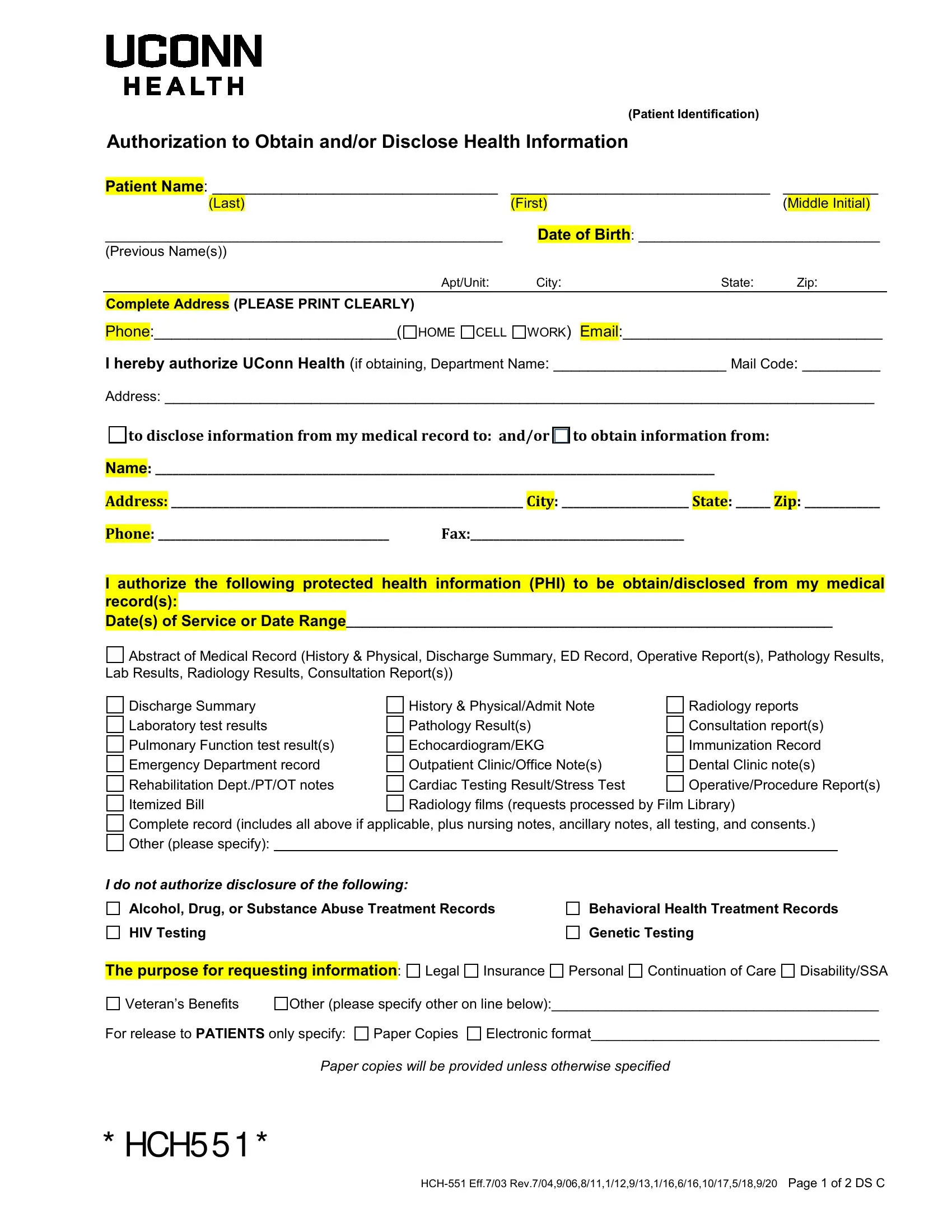
Authorization to Obtain and/or Disclose Health Information |
|
|
|
|
|
|
|
|
______________________________ |
___________ |
|
Patient Name |
: _________________________________ |
|
|
|
(Last) |
|
(First) |
|
|
( |
Middle Initial) |
|
|
|
|
|
___________________________________________________ |
|
Date of Birth |
: _______________________________ |
(Previous Name(s)) |
|
|
|
|
|
|
|
|
|
|
|
|
Apt/Unit: |
City: |
State: |
|
Zip: |
|
|
|
|
|
|
|
|
|
|
|
Complete Address |
(PLEASE PRINT CLEARLY) |
|
|
|
|
|
|
|
Phone:____________________________(
HOME CELL WORK) Email:______________________________
Ihereby authorize UConn Health (if obtaining, Department Name: ____________________ Mail Code: _________
Address: __________________________________________________________________________________
to disclose information from my medical record to: and/or to obtain information from:
Name: _________________________________________________________________________________________________
Address: _____________________________________________________________ City: ______________________ State: ______ Zip: _____________
Phone: ________________________________________ Fax:_____________________________________
I authorize the following protected health information (PHI) to be obtain/disclosed from my medical record(s):
Date(s) of Service or Date Range______________________________________________________________
Abstract of Medical Record (History & Physical, Discharge Summary, ED Record, Operative Report(s), Pathology Results,
Lab Results, Radiology Results, Consultation Report(s)) |
|
Discharge Summary |
History & Physical/Admit Note |
Radiology reports |
Laboratory test results |
Pathology Result(s) |
Consultation report(s) |
Pulmonary Function test result(s) |
Echocardiogram/EKG |
Immunization Record |
Emergency Department record |
Outpatient Clinic/Office Note(s) |
Dental Clinic note(s) |
Rehabilitation Dept./PT/OT notes |
Cardiac Testing Result/Stress Test |
Operative/Procedure Report(s) |
Itemized Bill |
Radiology films (requests processed by Film Library) |
Complete record (includes all above if applicable, plus nursing notes, ancillary notes, all testing, and consents.) Other (please specify):
I do not authorize disclosure of the following:
Alcohol, Drug, or Substance Abuse Treatment Records
HIV Testing
Behavioral Health Treatment Records
Genetic Testing
|
|
|
|
|
|
|
|
|
The purpose for requesting information |
: |
Legal |
Insurance |
Personal |
Continuation of Care |
Disability/SSA |
Veteran’s Benefits |
Other (please specify other on line below):__________________________________________ |
For release to PATIENTS only specify: |
Paper Copies |
Electronic format_____________________________________ |
Paper copies will be provided unless otherwise specified
* HCH5 5 1 *
HCH-551 Eff.7/03 Rev.7/04,9/06,8/11,1/12,9/13,1/16,6/16,10/17,5/18,9/20 Page 1 of 2 DS C
(Patient Identification)
Authorization to Obtain and/or Disclose Health Information
By signing this authorization form, I understand that:
•This authorization is voluntary and that my records may include protected information relating to AIDS, HIV testing and results, behavioral health treatment, treatment for alcohol ,drug and/or substance abuse.
•A patient whom is a minor (age 13 or older) must also sign the authorization, if medical records contain protected information with the exception of Behavioral Health, which requires authorization by the patient if a minor age 16 or older.
•Requests for copies of medical records are subject to fees as allowed by law.
•In cases where UConn Health is requested by a third party to create health information solely for sharing that information with the party that requested it, I understand that I must sign this authorization.
•I may change my mind and cancel (revoke) this authorization. I have the right to revoke this authorization at any time. This authorization may be revoked in writing to the Director of Health Information Management. It will not apply to information that has already been disclosed in response to this authorization.
•Unless otherwise revoked, this authorization will expire on the following date/event/condition:
_________________________________. If I fail to specify an expiration date/event/condition, this authorization will expire six (6) months from the date signed.
•I understand that the information disclosed under this authorization may be subject to further disclosure by the recipient and thus, may no longer be protected by federal privacy regulations.
•I understand that my treatment or continued treatment by UConn Health is in no way conditioned on whether or not I sign this authorization and that I may refuse to sign it.
•I understand that I may inspect or copy the information to be used or disclosed and that I may receive a copy of this signed authorization.
•If this disclosure contains information relating to HIV, behavioral health, alcohol, drug and/or substance abuse treatment, the following shall apply: This information has been disclosed to you from records whose confidentiality is protected by law. Federal regulations (Title 42 CFR Part 2) and Connecticut General Statutes (Ch. 368x) prohibit you from making any further disclosure of it without the specific written consent of the person to whom it pertains, or as otherwise permitted by such regulations. A general authorization for the release of psychiatric or substance abuse information is NOT sufficient for this purpose.
Return completed authorization via mail, fax or email (Patient use only) to:
Mailing Address: |
UConn Health |
|
|
|
|
|
|
Health Information Management |
|
Release of Information MC2260 |
|
263 Farmington Ave |
|
Farmington, CT 06030 |
ROI Office Fax Number: |
860-679-1273 |
|
|
|
|
|
Email (For Patient Use only): |
PatientROIRequests@uchc.edu |
___ |
|
|
_____________ |
Signature of Patient or Authorized Representative |
** |
|
|
|
Date/Time |
|
|
|
|
__ |
|
|
|
|
Printed name of Patient or Authorized Representative ** |
□Healthcare Representative □Conservator |
Relationship to Patient: □Self □Parent |
□ Legal Guardian |
□Executor/Administrator of Estate □ Power of Attorney
□Other Authorized Representative: _________________________________
** A copy of the authorized representative’s legal authority to act on behalf of the patient must be attached.
Name and relationship to patient of individual authorized to pick up record(s) being released from the facility:
____________________________________
Questions? Please call 860-679-2787
HCH-551 Eff.7/03 Rev.7/04,9/06,8/11,1/12,9/13,1/16,6/16,10/17,5/18,9/20 Page 2 of 2 DS C