
Using PDF files online is certainly surprisingly easy with our PDF editor. You can fill in ohio board of health complaints here without trouble. The tool is consistently maintained by our team, receiving additional functions and turning out to be much more convenient. To start your journey, take these easy steps:
Step 1: Just click on the "Get Form Button" in the top section of this webpage to launch our pdf form editing tool. Here you will find everything that is needed to work with your file.
Step 2: Using our advanced PDF editor, you may accomplish more than just fill in blank fields. Try each of the features and make your forms look faultless with customized textual content incorporated, or fine-tune the original input to excellence - all that comes with the capability to insert stunning images and sign the file off.
Pay attention while completing this document. Make sure that all necessary fields are filled in properly.
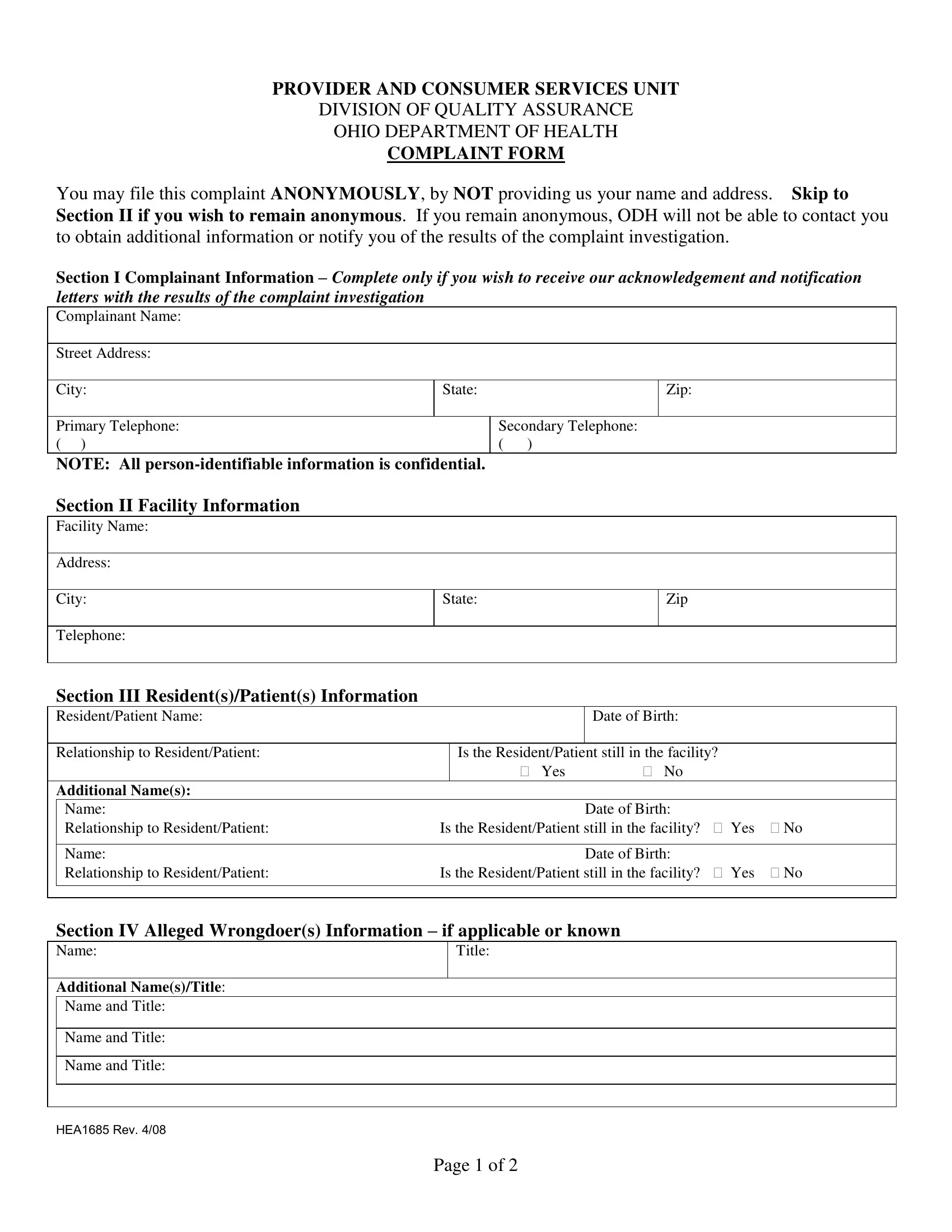
1. Start filling out your ohio board of health complaints with a selection of essential blank fields. Get all the necessary information and ensure there is nothing left out!
2. Just after this selection of blanks is completed, go to type in the relevant information in all these: Section III ResidentsPatients, Is the ResidentPatient still in, Additional Names, Name Date of Birth Relationship to, Name Date of Birth Relationship to, Section IV Alleged Wrongdoers, Title, Name and Title, Name and Title, Name and Title, and HEA Rev.
As to Name and Title and Section IV Alleged Wrongdoers, make sure you double-check them in this section. These two are certainly the most important fields in this form.
3. Completing Section V Narrative Description is essential for the next step, make sure to fill them out in their entirety. Don't miss any details!
Step 3: Reread everything you have typed into the blanks and then press the "Done" button. Go for a free trial plan with us and get immediate access to ohio board of health complaints - with all transformations kept and accessible in your personal cabinet. When using FormsPal, you can easily complete forms without worrying about information incidents or data entries being distributed. Our secure platform makes sure that your personal data is kept safely.