

Any time you want to fill out sun life claim form pdf, you won't have to install any kind of software - just try our online PDF editor. To make our tool better and more convenient to utilize, we consistently come up with new features, with our users' feedback in mind. Getting underway is simple! Everything you should do is adhere to the next simple steps below:
Step 1: Open the PDF form in our tool by pressing the "Get Form Button" at the top of this page.
Step 2: With our handy PDF file editor, you can do more than just fill in blanks. Express yourself and make your documents seem faultless with custom text put in, or modify the file's original content to excellence - all that comes with the capability to add stunning photos and sign the document off.
In order to complete this PDF form, make sure that you enter the necessary information in every single blank field:
1. First, once filling out the sun life claim form pdf, start with the area that contains the following blanks:
2. Just after finishing this section, go to the subsequent stage and complete all required particulars in all these blank fields - What is your employment status, m Fulltime m Parttime m Retired, If your other benefit plan is with, m No m Yes, Contract number, Member ID number, Information about your claim, List the names of all persons for, Fulltime student Disabled Amount, Relationship to you, Date of birth yyyymmdd, Last name, Last name, Last name, and Last name.
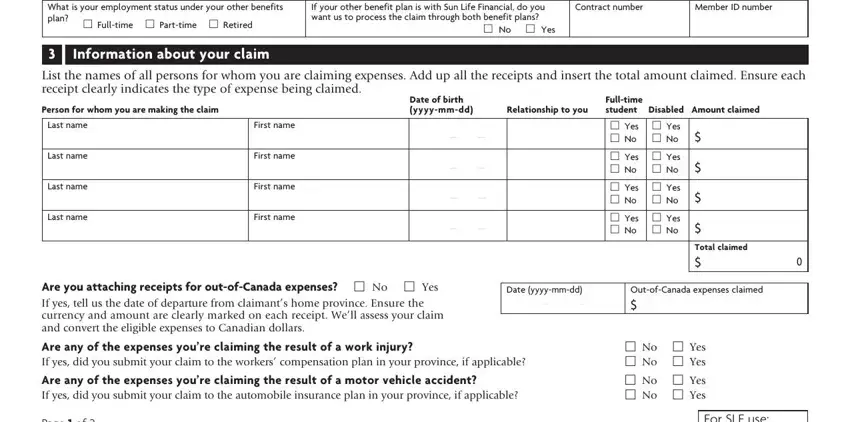
People frequently make mistakes while filling out Date of birth yyyymmdd in this area. Be sure you revise everything you enter here.
3. Completing Members signature, Respecting your privacy, Date yyyymmdd, Your privacy is important to us We, To find out about our Privacy, Questions Please visit, Mailing instructions keep a copy, Mail your completed form to the, Sun Life Assurance Company of, and Sun Life Assurance Company of is essential for the next step, make sure to fill them out in their entirety. Don't miss any details!
Step 3: Before moving on, make certain that form fields have been filled in correctly. When you think it's all fine, click “Done." Right after registering afree trial account here, you'll be able to download sun life claim form pdf or email it right off. The document will also be accessible via your personal account page with your every change. FormsPal provides safe form editor with no data recording or sharing. Rest assured that your details are in good hands with us!