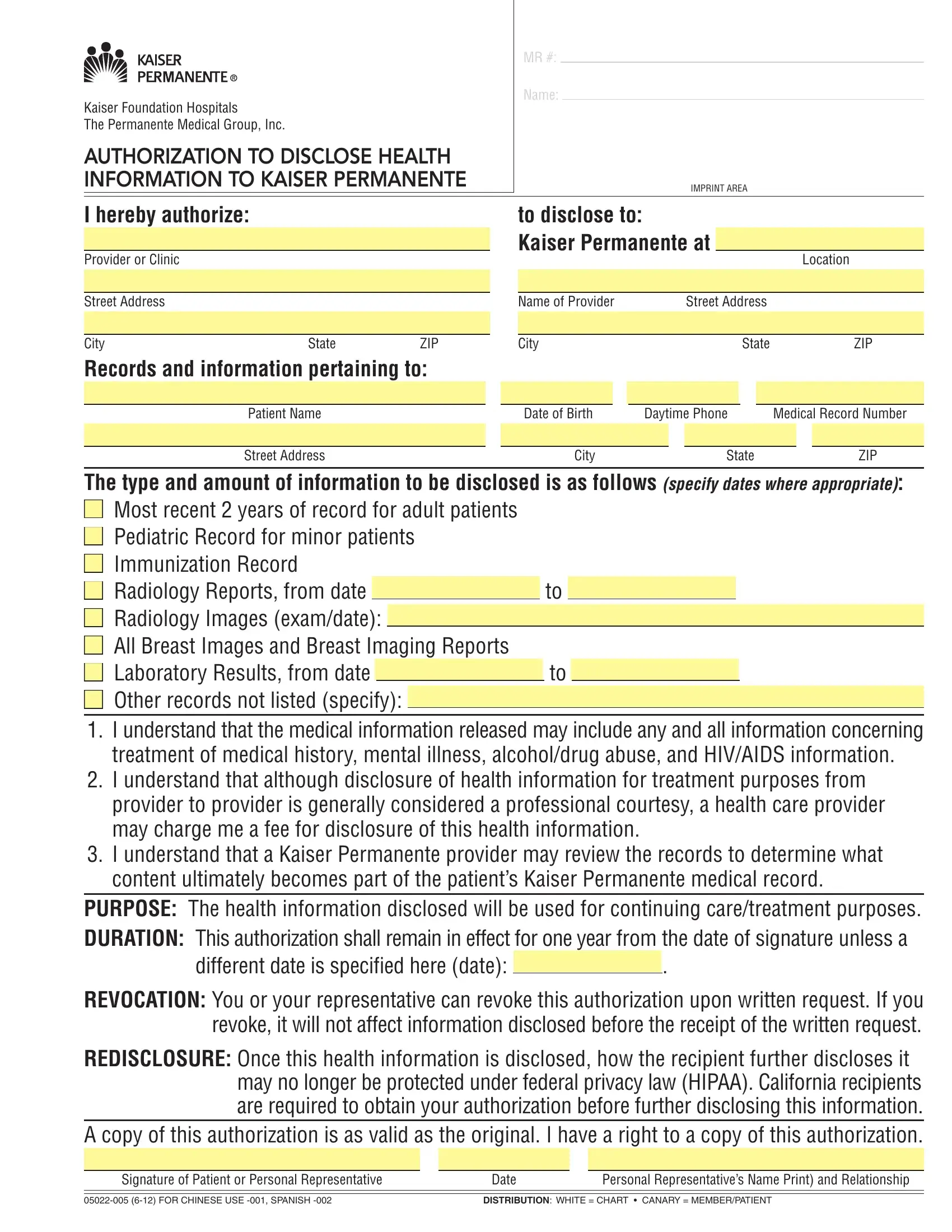
Navigating the complexities of sharing health information can be challenging, but the Health Information Kaiser Permanente form provides a structured and secure method for individuals to authorize the disclosure of their medical records. This form is an essential tool for patients of Kaiser Foundation Hospitals and The Permanente Medical Group, Inc., facilitating the seamless transfer of vital health information to Kaiser Permanente. It specifies the type and scope of records to be shared, ranging from the most recent two years of adult patient records to pediatric and immunization records, and even detailed reports like radiology and laboratory results. Importantly, the form addresses the inclusion of sensitive information, such as details of mental illness, alcohol or drug abuse, and HIV/AIDS, highlighting the comprehensive nature of the data transfer. Patients are made aware that while transferring records between providers is generally a courtesy, fees may apply, and they have the control to revoke the authorization at any time. The purpose behind this exchange is chiefly for the continuation of care or treatment, ensuring that healthcare providers have a full picture of the patient's medical history. Furthermore, this document outlines the protocol for how the information, once shared, will be incorporated into the patient’s Kaiser Permanente medical record, with a clear mention of how privacy is managed according to federal laws and California-specific regulations. The form underscores the patient's rights, including the ability to obtain a copy of the authorization, establishing a framework of trust and clarity in the sharing of health information.
| Question | Answer |
|---|---|
| Form Name | Health Information Kaiser Permanente Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | disclose information kaiser, medical kaiser disclosed, authorization disclose health information kaiser, health permanente information kaiser |
Kaiser Foundation Hospitals
The Permanente Medical Group, Inc.
AUTHORIZATION TO DISCLOSE HEALTH INFORMATION TO KAISER PERMANENTE
MR #:
Name:
|
|
|
IMPRINT AREA |
|
|
|
|
|
|
I hereby authorize: |
|
|
to disclose to: |
|
|
|
|
Kaiser Permanente at |
|
Provider or Clinic |
|
|
Location |
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
Street Address
City |
State |
ZIP |
Name of Provider |
Street Address |
|
|
|
|
|
|
|
City |
State |
ZIP |
Records and information pertaining to:
Patient Name |
|
Date of Birth |
Daytime Phone |
Medical Record Number |
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Street Address |
|
City |
|
|
State |
|
|
ZIP |
|
|
|
|
|
|
|
|
|
The type and amount of information to be disclosed is as follows (specify dates where appropriate):
■ Most recent 2 years of record for adult patients |
|
|
|
|||
■ Pediatric Record for minor patients |
|
|
|
|||
■ Immunization Record |
|
|
|
|||
■ Radiology Reports, from date |
|
|
|
to |
|
|
■ Radiology Images (exam/date): |
|
|
|
|
|
|
|
|
|
|
|
||
■ All Breast Images and Breast Imaging Reports |
|
|
|
|||
■ Laboratory Results, from date |
|
|
|
to |
|
|
■ Other records not listed (specify): |
|
|
|
|
||
|
|
|
|
|||
|
|
|
|
|
|
|
1.I understand that the medical information released may include any and all information concerning treatment of medical history, mental illness, alcohol/drug abuse, and HIV/AIDS information.
2.I understand that although disclosure of health information for treatment purposes from provider to provider is generally considered a professional courtesy, a health care provider may charge me a fee for disclosure of this health information.
3.I understand that a Kaiser Permanente provider may review the records to determine what content ultimately becomes part of the patient’s Kaiser Permanente medical record.
PURPOSE: The health information disclosed will be used for continuing care/treatment purposes.
DURATION: This authorization shall remain in effect for one year from the date of signature unless a
different date is speciied here (date): .
REVOCATION: You or your representative can revoke this authorization upon written request. If you revoke, it will not affect information disclosed before the receipt of the written request.
REDISCLOSURE: Once this health information is disclosed, how the recipient further discloses it may no longer be protected under federal privacy law (HIPAA). California recipients are required to obtain your authorization before further disclosing this information.
A copy of this authorization is as valid as the original. I have a right to a copy of this authorization.
Signature of Patient or Personal Representative |
Date |
Personal Representative’s Name Print) and Relationship |
|
|
|
|
|
|
DISTRIBUTION: WHITE = CHART • CANARY = MEMBER/PATIENT |
||