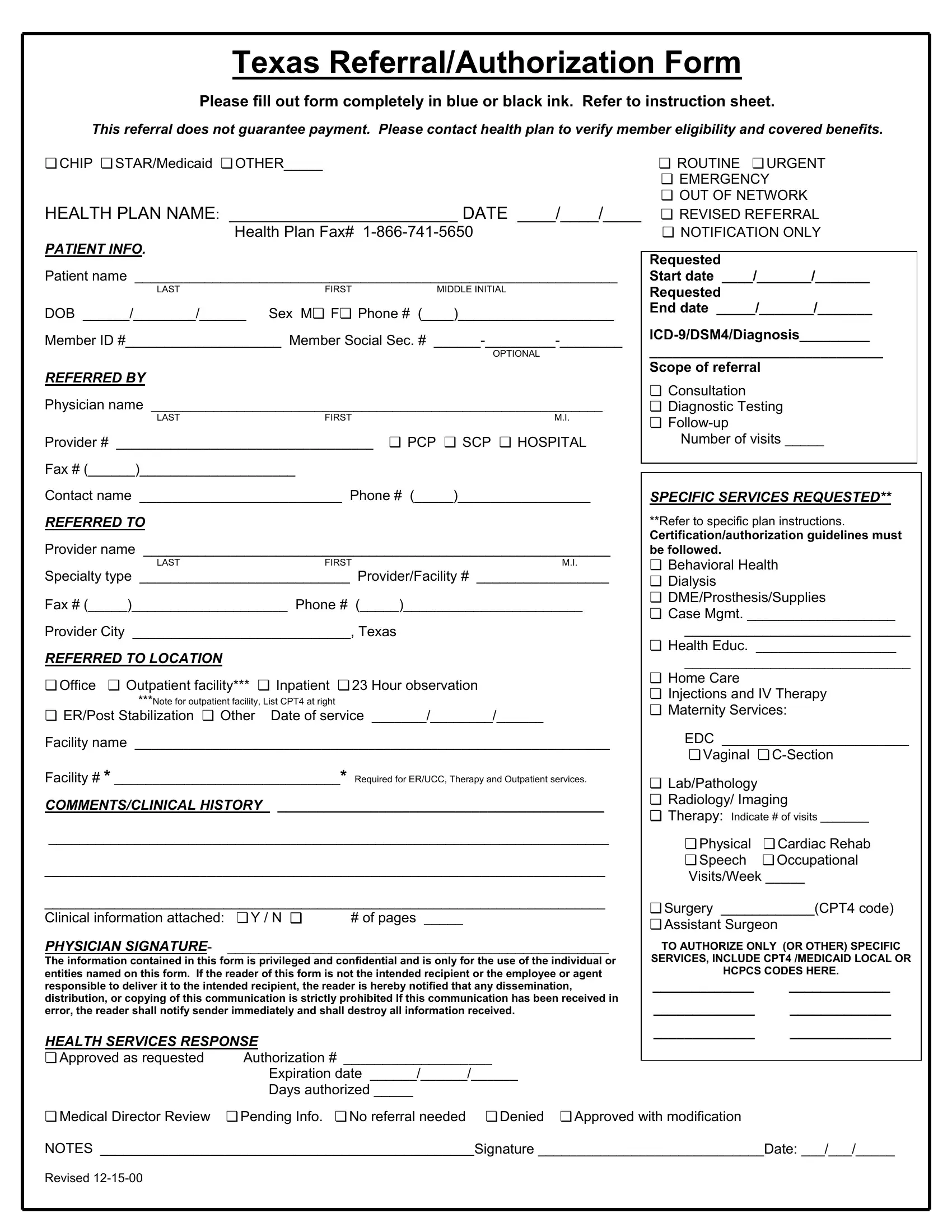
Navigating through the healthcare system can often feel like a maze, with each turn presenting a new challenge. One such challenge is when a patient or a healthcare provider feels the need to question or contest a decision made by a health plan. This is where the Health Plan Appeal form plays a crucial role. Designed as a formal request for review, this document is filled out with details such as patient information, referring and referred physicians, and specific services requested, all aimed at persuading the health plan to reconsider its initial decision. It's a document that demands meticulous attention to detail - from ensuring all sections are completed in blue or black ink to attaching any necessary clinical information. The form underscores the importance of verifying member eligibility and understanding that a referral does not guarantee payment. It brings to light the various ways in which care can be sought, underlining the significance of specifying the type of service requested, be it for behavioral health, maternity services, or surgery among others. Moreover, the appeal process underscores the health plan's response options, which range from approval to denial, and highlights the urgency levels that can be marked, illustrating the form's flexibility in accommodating various patient needs. This form serves not only as a means to challenge an unfavorable decision but also as a reflection of the intricate web of policies, procedures, and regulations that govern healthcare services.
| Question | Answer |
|---|---|
| Form Name | Health Plan Appeal Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | driscoll childrens chips appeal form, driscoll health plan prior authorization form, driscoll prior authorization form pdf, driscoll health plan authorization phone number |
Texas Referral/Authorization Form
Please fill out form completely in blue or black ink. Refer to instruction sheet.
This referral does not guarantee payment. Please contact health plan to verify member eligibility and covered benefits.
❏CHIP ❏ STAR/Medicaid ❏ OTHER_____
HEALTH PLAN NAME: |
________________________ DATE ____/____/____ |
|
|
Health Plan Fax# |
|
PATIENT INFO. |
|
|
|
|
|
Patient name ______________________________________________________________ |
||
LAST |
FIRST |
MIDDLE INITIAL |
DOB ______/________/______ Sex M❏ F❏ Phone # (____)____________________ |
||
Member ID #____________________ Member Social Sec. # |
||
|
|
OPTIONAL |
REFERRED BY |
|
|
Physician name __________________________________________________________ |
||
LAST |
FIRST |
M.I. |
Provider # _________________________________ |
❏ PCP ❏ SCP ❏ HOSPITAL |
|
|
|
|
Fax # (______)____________________
Contact name __________________________ Phone # (_____)_________________
REFERRED TO
Provider name ____________________________________________________________
LASTFIRSTM.I.
Specialty type ___________________________ Provider/Facility # _________________
Fax # (_____)____________________ Phone # (_____)_______________________
Provider City ____________________________, Texas
REFERRED TO LOCATION
❏Office ❏ Outpatient facility*** ❏ Inpatient ❏ 23 Hour observation
***Note for outpatient facility, List CPT4 at right
❏ ER/Post Stabilization ❏ Other Date of service _______/________/______
Facility name _____________________________________________________________
Facility # * _____________________________* Required for ER/UCC, Therapy and Outpatient services.
COMMENTS/CLINICAL HISTORY __________________________________________
________________________________________________________________________
________________________________________________________________________
________________________________________________________________________
Clinical information attached: |
❏ Y / N ❏ |
# of pages _____ |
PHYSICIAN SIGNATURE- |
_________________________________________________ |
|
The information contained in this form is privileged and confidential and is only for the use of the individual or entities named on this form. If the reader of this form is not the intended recipient or the employee or agent responsible to deliver it to the intended recipient, the reader is hereby notified that any dissemination, distribution, or copying of this communication is strictly prohibited If this communication has been received in error, the reader shall notify sender immediately and shall destroy all information received.
HEALTH SERVICES RESPONSE
❏ Approved as requested |
Authorization # ___________________ |
|
Expiration date ______/______/______ |
|
Days authorized _____ |
❏ROUTINE ❏ URGENT
❏EMERGENCY
❏OUT OF NETWORK
❏REVISED REFERRAL
❏NOTIFICATION ONLY
Requested
Start date ____/_______/_______
Requested
End date _____/_______/_______
______________________________
Scope of referral
❏Consultation
❏Diagnostic Testing
❏
Number of visits _____
SPECIFIC SERVICES REQUESTED**
**Refer to specific plan instructions.
Certification/authorization guidelines must be followed.
❏Behavioral Health
❏Dialysis
❏DME/Prosthesis/Supplies
❏Case Mgmt. ___________________
_____________________________
❏Health Educ. __________________
_____________________________
❏Home Care
❏Injections and IV Therapy
❏Maternity Services:
EDC ________________________
❏ Vaginal ❏
❏Lab/Pathology
❏Radiology/ Imaging
❏Therapy: Indicate # of visits ________
❏Physical ❏ Cardiac Rehab
❏Speech ❏ Occupational Visits/Week _____
❏Surgery ____________(CPT4 code)
❏Assistant Surgeon
TO AUTHORIZE ONLY (OR OTHER) SPECIFIC SERVICES, INCLUDE CPT4 /MEDICAID LOCAL OR HCPCS CODES HERE.
_____________ |
_____________ |
_____________ |
_____________ |
_____________ |
_____________ |
❏ Medical Director Review ❏ Pending Info. ❏ No referral needed ❏ Denied ❏ Approved with modification
NOTES ________________________________________________Signature _____________________________Date: ___/___/_____
Revised