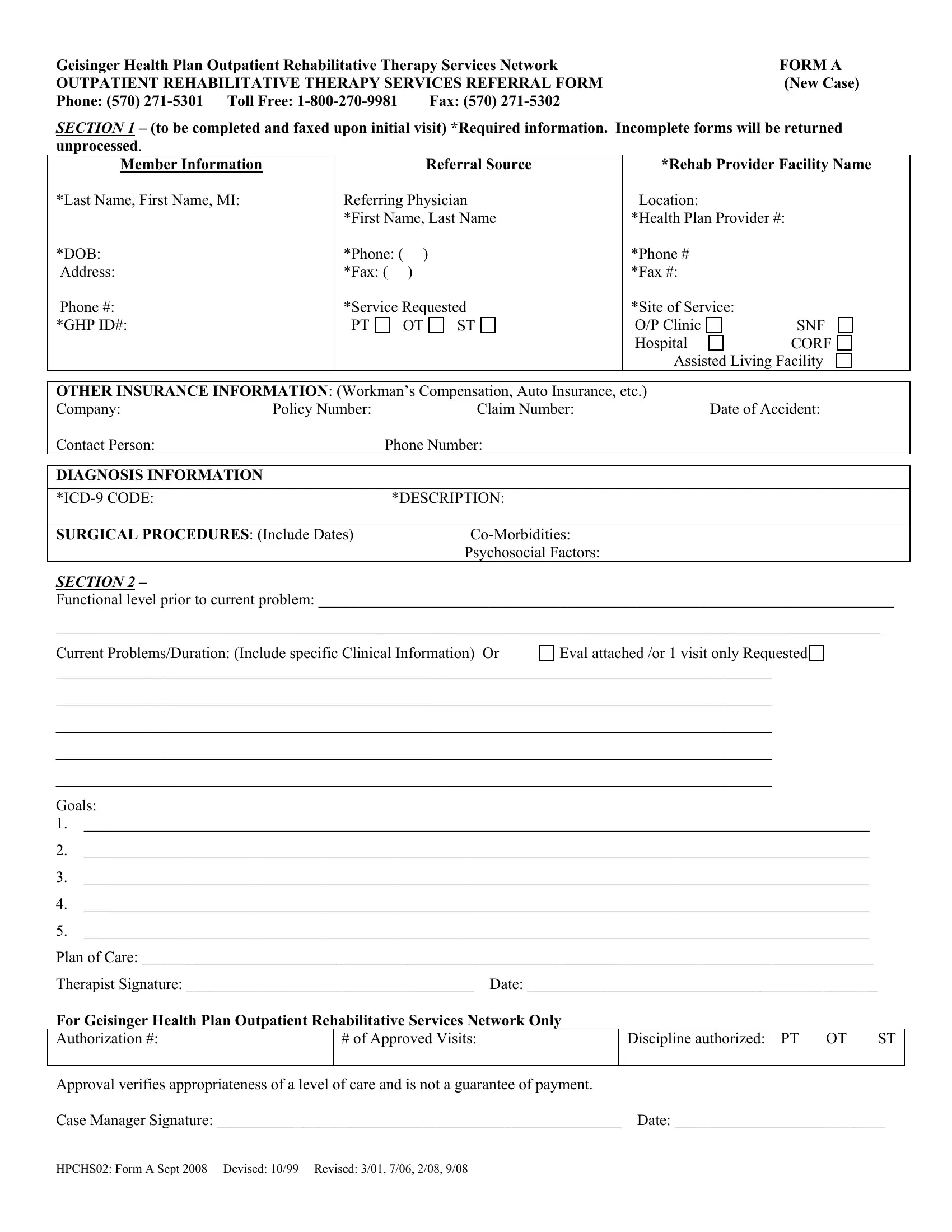
When individuals seek outpatient rehabilitative therapy services through the Geisinger Health Plan, they encounter a key document known as Form A. This essential paperwork initiates the referral process for new cases, ensuring that members get the targeted rehabilitation they need, whether that's physical therapy (PT), occupational therapy (OT), speech therapy (ST), or other specialized services. The form requires detailed information right from the start, including member and referral source details, the specific rehabilitation provider involved, and crucial member data such as their health plan provider number and date of birth. Furthermore, it addresses the necessity of documenting other insurance details, possibly indicating workman's compensation or auto insurance, alongside a comprehensive section dedicated to diagnosing information, including ICD-9 codes and descriptions of surgical procedures. The form also delves into the patient’s functional level prior to their current issue, outlines current problems and durations, and charts out goals and a plan of care, all of which are foundational in forming a tailored, patient-centric rehabilitation program. This exhaustive documentation process, underscored by the need for thoroughness and accuracy, not only facilitates a seamless referral but also ensures that the care provided aligns with the patient's specific rehabilitation needs. The form concludes with sections for therapist and case manager signatures, which validate the planned course of treatment and authorize the number of visits, emphasizing that while approval signifies the appropriateness of care level, it does not guarantee payment.
| Question | Answer |
|---|---|
| Form Name | Geisinger Health Plan Form A |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | CORF, appropriateness, 2008, Workmans |