Managing documents along with our PDF editor is easier when compared with nearly anything. To edit medicare health risk assessment questionnaire the file, there is nothing you have to do - just follow the actions down below:
Step 1: To begin, select the orange button "Get Form Now".
Step 2: You can now modify the medicare health risk assessment questionnaire. You need to use our multifunctional toolbar to add, eliminate, and transform the text of the file.
Fill out the medicare health risk assessment questionnaire PDF and enter the information for every single section:
Enter the required data in What is your preferred language, q English q Russian, q Somali q Swahili, q Spanish q French, q Arabic q Mandarin, What is your gender, q Male, q Female, q Vietnamese q Bosnian q Sign, q Other, What is your race optional q, What is your ethnicity optional q, q NonHispanic, q Asian q Declined to Answer, and q Black or African American area.
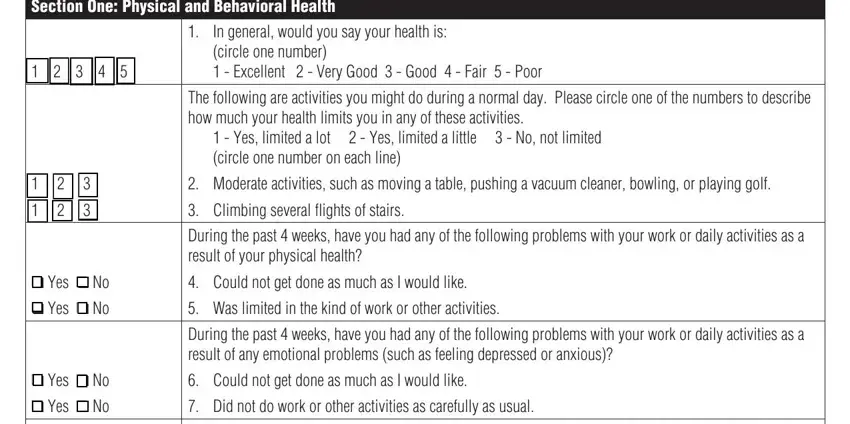
You will be requested for some fundamental details in order to complete the Section One Physical and, In general would you say your, circle one number Excellent, The following are activities you, Yes limited a lot Yes limited, Moderate activities such as, Climbing several flights of stairs, During the past weeks have you, q Yes q No q Yes q No, Could not get done as much as I, Was limited in the kind of work, During the past weeks have you, q Yes q No q Yes q No, Could not get done as much as I, and Did not do work or other segment.
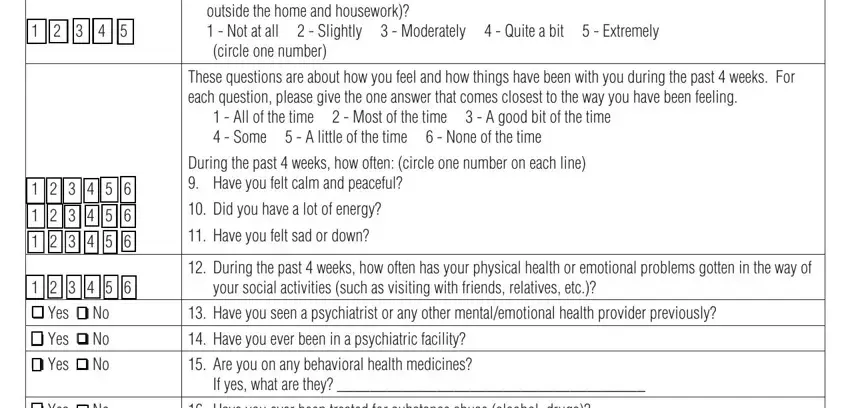
The During the past weeks how much, outside the home and housework, These questions are about how you, All of the time Most of the, During the past weeks how often, Did you have a lot of energy, Have you felt sad or down, During the past weeks how often, your social activities such as, Have you seen a psychiatrist or, Have you ever been in a, Are you on any behavioral health, If yes what are they, Have you ever been treated for, and q Yes q No q Yes q No q Yes segment allows you to point out the rights and obligations of all sides.
Finish by looking at the next sections and preparing them as required: Have you ever been treated for, Do you need help getting a, Do you need help getting food, and q Yes q No q Yes q No q Yes q No.
Step 3: Click the "Done" button. Now it's easy to export the PDF file to your gadget. Aside from that, you can send it by electronic mail.
Step 4: Produce no less than several copies of the form to stay clear of any specific possible future issues.
