This PDF editor was built with the objective of allowing it to be as effortless and intuitive as possible. The following steps are going to make filling out the health screening report sample simple.
Step 1: The following web page contains an orange button saying "Get Form Now". Please click it.
Step 2: The document editing page is currently open. Include information or manage existing details.
Create the following parts to create the document:
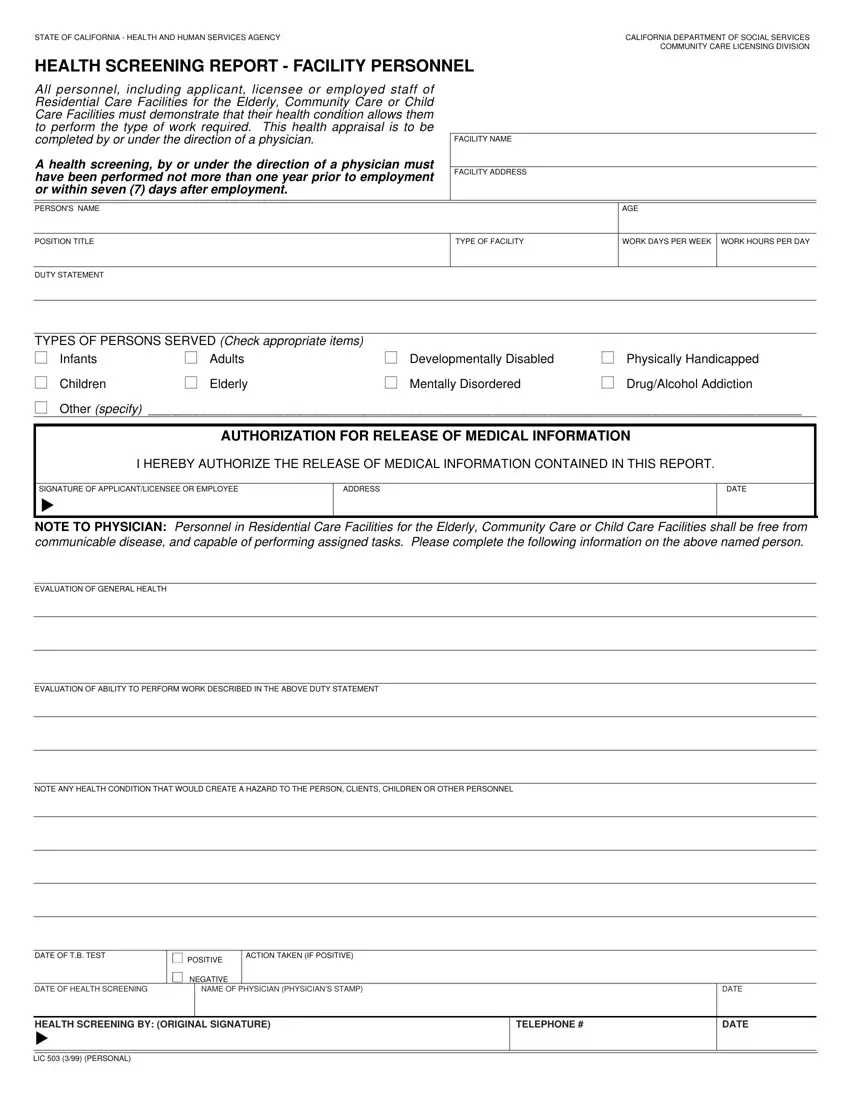
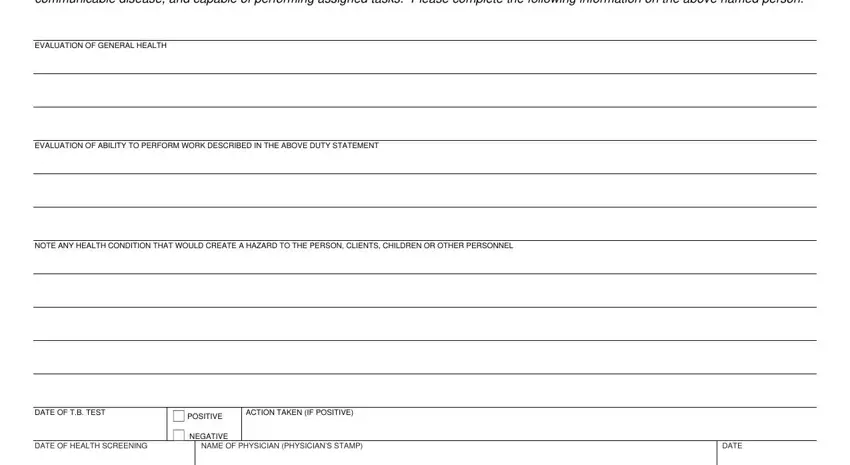
The software will require you to submit the NOTE TO PHYSICIAN Personnel in, EVALUATION OF GENERAL HEALTH, EVALUATION OF ABILITY TO PERFORM, NOTE ANY HEALTH CONDITION THAT, DATE OF TB TEST, ACTION TAKEN IF POSITIVE, POSITIVE, NEGATIVE, DATE OF HEALTH SCREENING, NAME OF PHYSICIAN PHYSICIANS STAMP, and DATE box.
Write down the crucial information in HEALTH SCREENING BY ORIGINAL, TELEPHONE, LIC PERSONAL, and DATE area.

Step 3: Hit the button "Done". The PDF document may be exported. It is possible to upload it to your computer or send it by email.
Step 4: To avoid any kind of complications in the long run, you should have a minimum of several duplicates of your document.
