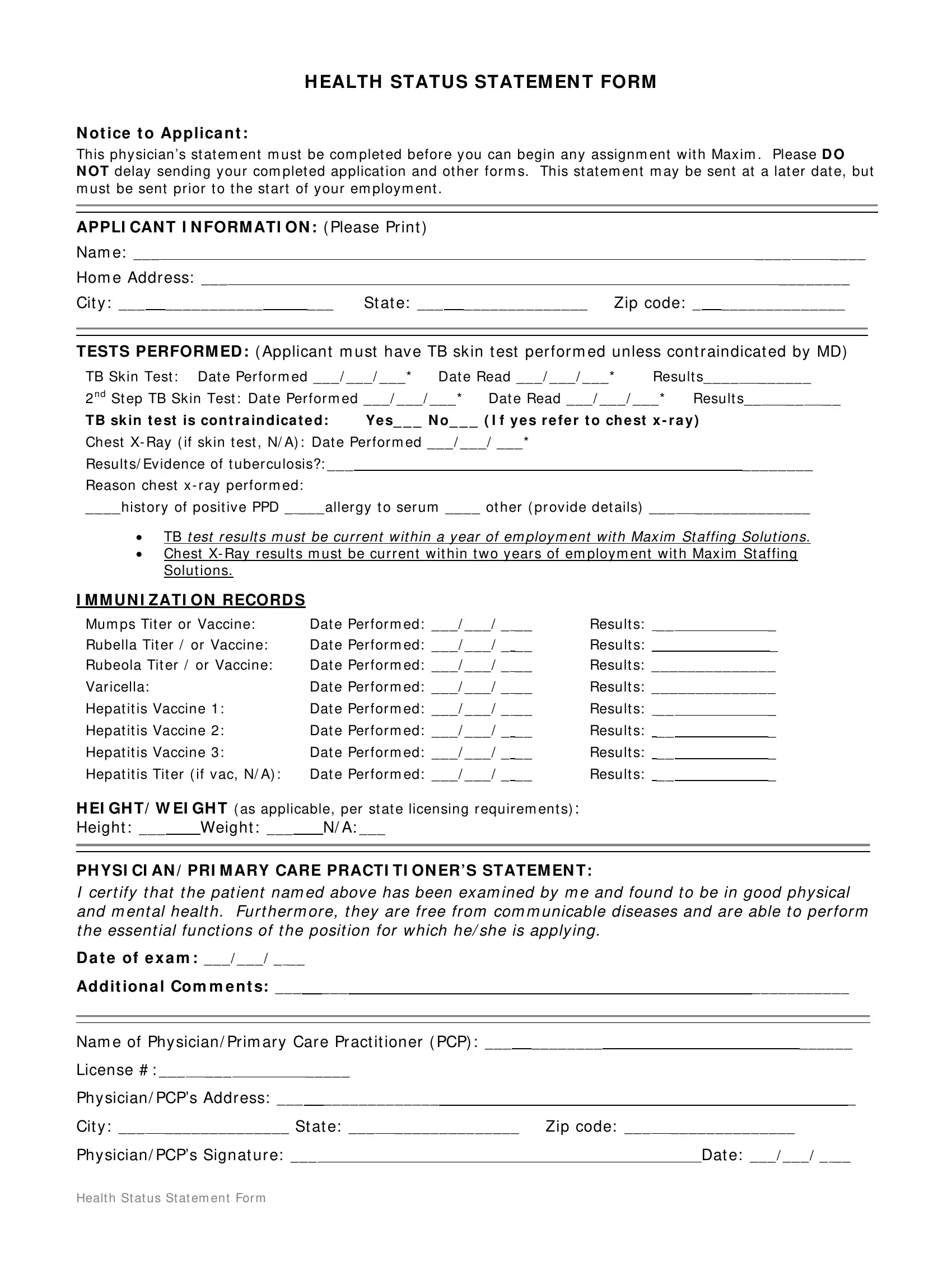
Before an individual can start their journey with Maxim, a rigorous health assessment, outlined in the Health Status Statement Form, is a prerequisite. This document serves as a comprehensive record, detailing the applicant's overall health and immunization history, a critical step for ensuring the safety and wellness of both the employee and those they will serve. At the heart of the form is the physician's statement, which certifies the applicant's physical and mental fitness for the position they are applying for. Additionally, the form mandates current tuberculosis (TB) testing, either through skin tests or, if contraindicated, a chest X-Ray, alongside a historical immunization record which includes, but is not limited to, mumps, rubella, rubeola, and varicella titers or vaccines, as well as a series of hepatitis vaccines or titers. The precise requirements for height and weight measurements further underscore the importance of meeting state licensing requirements. By submitting this form completed by a qualified healthcare professional, applicants demonstrate their readiness and eligibility for employment, underlining Maxim's commitment to high health and safety standards.
| Question | Answer |
|---|---|
| Form Name | Health Status Statement Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | 2nd, PCPs, what to write in health status, health status form |
H EALTH STATU S STATEM EN T FORM
N ot ice t o Applica n t :
This phy sician’s st at em ent m ust be com plet ed befor e y ou can begin any assignm ent w it h Max im . Please D O
N OT delay sending y our com plet ed applicat ion and ot her for m s. This st at em ent m ay be sent at a lat er dat e, but m ust be sent pr ior t o t he st ar t of y our em ploy m ent .
APPLI CAN T I N FORM ATI ON : ( Please Pr int )
Nam e: ___ |
|
|
|
|
|
|
|
____ |
|
____ |
||||||
Hom e Addr ess: ___ |
|
|
|
|
|
|
|
________ |
||||||||
Cit y : ___ ___________ |
___ |
St at e: ___ ______________ |
Zip code: _ ______________ |
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
TESTS PERFORM ED : ( Applicant m ust hav e TB sk in t est per for m ed unless cont r aindicat ed by MD)
TB Skin Test : Dat e Per for m ed ___ / ___ / ___ * |
Dat e Read ___ / ___ / ___ * |
Result s____ ______ |
||||||||
2 n d St ep TB Sk in Test : Dat e Per for m ed ___ / ___ / ___ * |
|
|
|
|
|
|
|
|
||
Dat e Read ___ / ___ / ___ * |
Result s__ __ __ |
|||||||||
|
|
|
|
|
|
|
|
|
|
|
TB sk in t e st is con t r a in d ica t e d : Ye s_ _ _ N o _ _ _ ( I f y e s r e f e r t o ch e st x - r a y )
Chest X- Ray ( if sk in t est , N/ A) : Dat e Per for m ed ___ / ___ / ___ * |
|
|
|
|||
Result s/ Ev idence of t uber culosis?: ___ |
|
|
________ |
|||
Reason chest x - r ay per for m ed: |
|
|
|
|||
____ hist or y of posit iv e PPD _ ___ aller gy t o ser um ____ ot her ( pr ov ide det ails) ___ |
_____________ |
|||||
|
|
|
|
|
|
|
• TB t est r esult s m ust be cur r ent w it hin a y ear of em ploy m ent w it h Max im St affing Solut ions.
•Chest X- Ray r esult s m ust be cur r ent w it hin t w o y ear s of em ploy m ent w it h Max im St affing Solut ions.
I M M U N I ZATI ON RECORD S
Mum ps Tit er or Vaccine: |
Dat e Per for m ed: ___ / ___ / _ __ |
Result s: |
__ |
_ |
|||||||
|
|
|
|
|
|
|
|
|
|||
Rubella Tit er / or Vaccine: |
Dat e Per for m ed: ___ / ___ / _ __ |
Result s: |
|
_ |
|||||||
|
|
|
|
|
|
|
|||||
Rubeola Tit er / or Vaccine: |
Dat e Per for m ed: ___ / ___ / _ __ |
Result s: ______________ |
|||||||||
|
|
|
|
|
|
|
|||||
Var icella: |
|
|
Dat e Per for m ed: ___ / ___ / _ __ |
Result s: ______________ |
|||||||
|
|
|
|
|
|
|
|||||
Hepat it is Vaccine 1: |
Dat e Per for m ed: ___ / ___ / _ __ |
Result s: |
__ |
_ |
|||||||
|
|
|
|
|
|
|
|
||||
Hepat it is Vaccine 2: |
Dat e Per for m ed: ___ / ___ / _ __ |
Result s: |
__ |
_ |
|||||||
|
|
|
|
|
|
|
|
||||
Hepat it is Vaccine 3: |
Dat e Per for m ed: ___ / ___ / _ __ |
Result s: |
__ |
_ |
|||||||
|
|
|
|
|
|
|
|
||||
Hepat it is Tit er ( if v ac, N/ A) : |
Dat e Per for m ed: ___ / ___ / _ __ |
Result s: |
__ |
_ |
|||||||
|
|
|
|
|
|
|
|
||||
H EI GH T/ W EI GH T ( as applicable, per st at e licensing r equir em ent s) : |
|
|
|
|
|
||||||
Height : ___ |
|
Weight : ___ |
N/ A: ___ |
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PH YSI CI AN / PRI M ARY CARE PRACTI TI ON ER’S STATEM EN T:
I cer t ify t h at t h e pat ient n am ed abov e has been ex am ined by m e and found t o be in good ph y sical and m ent al healt h . Fur t her m or e, t hey ar e fr ee fr om com m unicable diseases and ar e able t o per for m t h e essent ial fu n ct ion s of t h e posit ion for w hich h e/ sh e is apply in g.
D a t e of e x a m : ___ / ___ / _ __ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Ad dit ion a l Com m e n t s: ___ |
|
|
___ |
|
|
|
|
|
|
|
|
___________ |
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
Nam e of Phy sician/ Pr im ar y Car e Pr act it ioner ( PCP) : ___ |
________ |
|
______ |
||||||||||||||||||||||
License # : ___ ___ |
_____ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
Phy sician/ PCP’s Addr ess: ___ |
|
_____________ |
|
|
|
|
|
_ |
|||||||||||||||||
Cit y : ___ ______________ St at e: ___ ______________ |
Zip code: ___ |
______________ |
|
|
|
|
|||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
Phy sician/ PCP’s Signat ur e: ___ |
|
|
|
|
|
Dat e: ___ / ___ / _ __ |
|||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Healt h St at us St at em ent For m