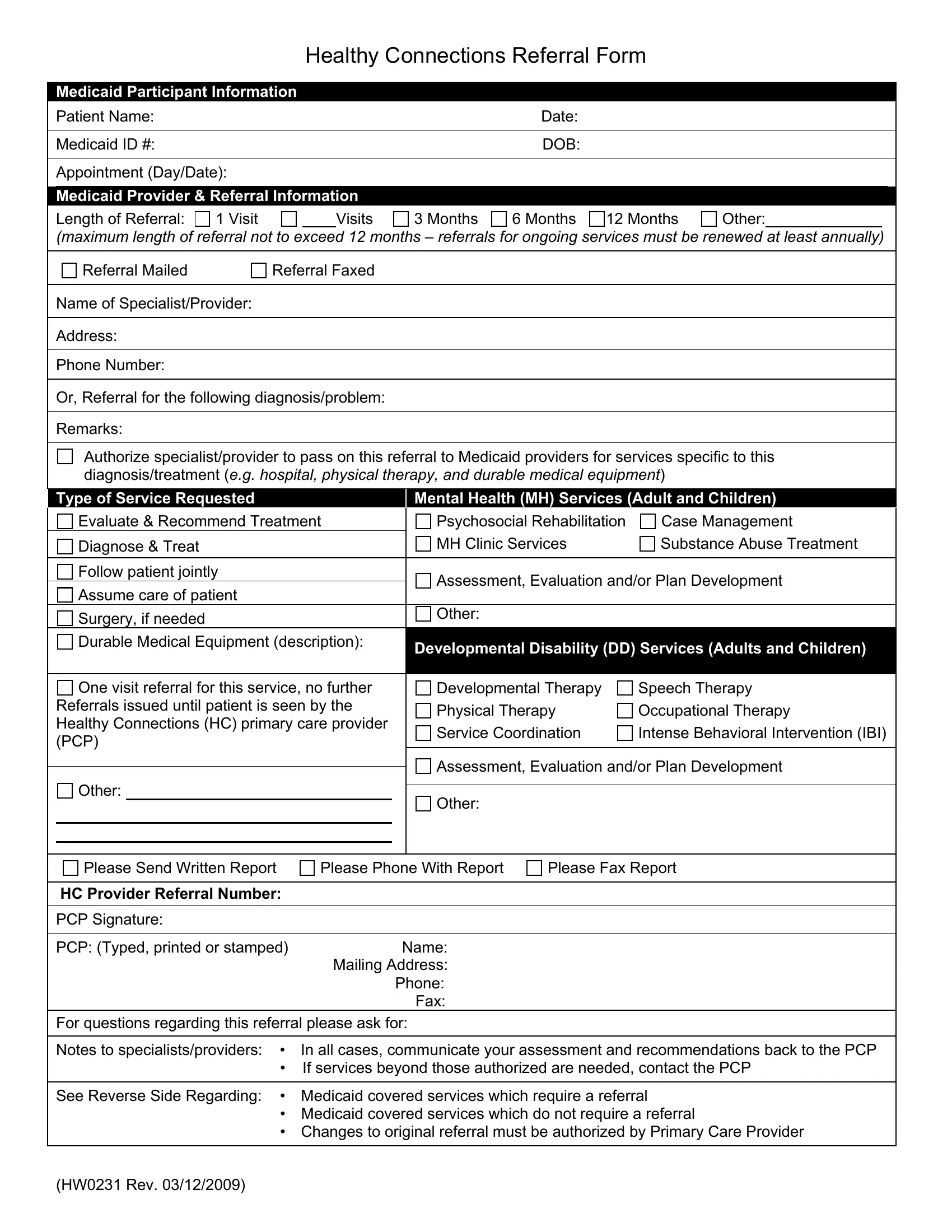
Ensuring timely and appropriate medical care for Medicaid participants is vital. The Healthy Connections Referral Form plays a crucial role in this process, bridging the gap between primary care providers (PCPs) and specialized medical services. This meticulously designed form captures essential Medicaid Participant Information, including the patient’s name, Medicaid ID, date of birth, and specifics about the appointment. It ventures further to encompass Medicaid Provider & Referral information, detailing the length of the referral—from a single visit up to a maximum of 12 months—and method of referral transmission, whether mailed or faxed. Important, too, is the inclusion of the specialist/provider's contact details and the type of service requested, which can range from mental health and substance abuse treatment to surgery and durable medical equipment needs. Notably, the form facilitates a streamlined communication line back to the PCP, mandating that specialists and providers share assessments and recommendations, vital for continuous patient care. For referrals surpassing the authorized services, re-initiating contact with the PCP is a procedural step indicated on the form. Additional components highlight services requiring a referral from the Healthy Connections PCP, contrasting with those services exempt from this requirement, illuminating the comprehensive nature of this instrumental form. Its strategic format and the detailed guidance it provides underscore its significance in the coordinated care ecosystem, ensuring Medicaid participants receive the necessary care, tailored to their specific health needs.
| Question | Answer |
|---|---|
| Form Name | Healthy Connections Referral Form |
| Form Length | 2 pages |
| Fillable? | Yes |
| Fillable fields | 59 |
| Avg. time to fill out | 12 min 22 sec |
| Other names | hw0231, healthy connections idaho, child and family connections referral form, children and family connection referral form |
|
|
Healthy Connections Referral Form |
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
Medicaid Participant Information |
|
|
|
|
|
|
|
|
Patient Name: |
|
|
|
Date: |
|
|
|
|
|
|
|
|
|
|
|
|
|
Medicaid ID #: |
|
|
|
DOB: |
|
|
|
|
|
|
|
|
|
|
|
|
|
Appointment (Day/Date): |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Medicaid Provider & Referral Information |
|
|
|
|
|
||
|
Length of Referral: 1 Visit |
|
Visits |
3 Months |
6 Months 12 Months |
Other: |
||
|
|
|
|
|
|
|
|
|
(maximum length of referral not to exceed 12 months – referrals for ongoing services must be renewed at least annually)
Referral Mailed |
Referral Faxed |
Name of Specialist/Provider:
Address:
Phone Number:
Or, Referral for the following diagnosis/problem:
Remarks:
Authorize specialist/provider to pass on this referral to Medicaid providers for services specific to this diagnosis/treatment (e.g. hospital, physical therapy, and durable medical equipment)
|
Type of Service Requested |
|
|
Mental Health (MH) Services (Adult and Children) |
|
|||
|
Evaluate & Recommend Treatment |
|
|
Psychosocial Rehabilitation |
Case Management |
|||
|
Diagnose & Treat |
|
|
MH Clinic Services |
Substance Abuse Treatment |
|||
|
|
|
|
|
|
|
|
|
|
Follow patient jointly |
|
|
Assessment, Evaluation and/or Plan Development |
||||
|
Assume care of patient |
|
|
|||||
|
|
|
|
|
|
|||
|
Surgery, if needed |
|
|
Other: |
|
|
||
|
|
|
|
|
|
|||
|
Durable Medical Equipment (description): |
|
|
Developmental Disability (DD) Services (Adults and Children) |
|
|||
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
One visit referral for this service, no further |
|
|
Developmental Therapy |
Speech Therapy |
|||
|
Referrals issued until patient is seen by the |
|
|
Physical Therapy |
Occupational Therapy |
|||
|
Healthy Connections (HC) primary care provider |
|
|
|||||
|
|
|
Service Coordination |
Intense Behavioral Intervention (IBI) |
||||
|
(PCP) |
|
|
|||||
|
|
|
|
|
|
|||
|
|
|
|
|
|
Assessment, Evaluation and/or Plan Development |
||
|
Other: |
|
|
|||||
|
|
|
|
|
|
|||
|
|
|
Other: |
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Please Send Written Report
Please Phone With Report
Please Fax Report
HC Provider Referral Number:
PCP Signature:
PCP: (Typed, printed or stamped) |
Name: |
|
Mailing Address: |
|
Phone: |
|
Fax: |
For questions regarding this referral please ask for:
Notes to specialists/providers: • In all cases, communicate your assessment and recommendations back to the PCP
•If services beyond those authorized are needed, contact the PCP
See Reverse Side Regarding: • Medicaid covered services which require a referral
•Medicaid covered services which do not require a referral
•Changes to original referral must be authorized by Primary Care Provider
(HW0231 Rev. 03/12/2009)
The following services require a referral from the Healthy Connections Primary Care Provider (PCP)
• |
Ambulatory Surgical Center Services |
|
• |
Oxygen and Related Services |
• |
Case Management |
|
• |
Physician Services: Not provided by the Healthy Connections |
• |
Developmental Therapy |
|
|
(HC) PCP. Including any |
|
|
services. |
||
• |
|
|
|
|
Durable Medical Equipment and Supplies (DME) |
• |
Physical Therapy |
||
• |
|
|
||
Home Health Service |
|
• Prosthetic and Orthotic Services |
||
• |
|
|
||
Hospice Services |
|
• |
Psychosocial Rehabilitation Services |
|
• |
|
|
||
Hospital Services: Inpatient and outpatient |
services. |
• |
Service Coordination |
|
|
(Some inpatient stays require PA through Qualis Health) |
|||
|
• |
|
||
• |
Intensive Behavioral Intervention (IBI) |
|
Speech Therapy |
|
|
• Substance Abuse Treatment Services |
|||
• |
Mental Health Clinic Services |
|
||
|
• |
|
||
• |
Occupational Therapy |
|
Urgent Care Centers |
|
|
|
|
||
|
|
|
|
|
Note: Some services require a prior authorization (PA) from the Department and a referral from the Healthy Connections PCP. For more information regarding Healthy Connections referral requirements, please refer to your Idaho Medicaid Provider Handbook.
The following services do not require a referral from the Healthy Connections Primary Care Provider (PCP)
• |
Anesthesiology |
• |
||
• |
Audiology Services (Performed in the office of a certified |
|
intermediate care facility requires authorization from the |
|
|
department. |
|||
|
audiologist) |
|
||
|
• Personal Care Services: Requires PA from the |
|||
• |
Chiropractic Services (Performed in the office) Medicaid |
|||
|
department. |
|||
|
does not reimburse chiropractors for |
|
||
|
• Personal Care Service Coordination: Requires PA |
|||
• |
Dental Services |
|||
|
from the department. |
|||
• |
|
|
||
Emergency Services (Performed in an |
• Pharmacy Services: For prescription drugs only. |
|||
|
emergency department of a hospital) |
|||
|
|
DME provided by pharmacies such as infusion |
||
• |
|
|
||
Family Planning Services: Counseling and |
|
pumps will require a referral and may require a PA |
||
|
supplies to prevent pregnancy. |
|
from the department. |
|
• |
Home and Community Bases Services (Waiver): |
• |
Podiatry Services: Performed in the office. Services |
|
|
Requires PA from the department. |
|
provided outside the Podiatrist’s office (hospital or ambulatory |
|
• |
Immunizations: Only when vaccine(s) is billed alone or in |
|
surgery center) will require a referral from the PCP. |
|
• |
|
|||
|
conjunction with an administration fee. Specialty |
Radiological Services. |
||
|
physicians/providers administering immunizations are |
• |
||
|
asked to provide the participant's PCP with immunization |
|||
|
|
services delivered by a school district or the |
||
|
records to assure continuity of care and avoid duplication |
|
||
|
|
Infant/Toddler Program. |
||
|
of services. |
|
||
|
• Screening Mammographies: Limited to one per |
|||
• |
Indian Health Clinic Services |
|||
|
calendar year for women age 40 or older. |
|||
• |
|
|
||
Influenza Shots Pneumococcal Vaccine: Only when |
• Sexually Transmitted Disease: Diagnosis and/or treatment. |
|||
|
vaccine is billed alone or in conjunction with an |
|||
|
• |
|
||
|
administration fee. |
Vision Services: Performed in the offices of |
||
• |
Laboratory and Pathology Services |
|
ophthalmologists and optometrists, including eye |
|
|
glasses. This does not include services performed in |
|||
|
|
|
||
|
|
|
a hospital or ambulatory surgery |
|
|
|
|
|
|
For more information on Idaho Medicaid requirements, please refer to your Idaho Medicaid Provider Handbook.
(HW0231 Rev. 03/12/2009)