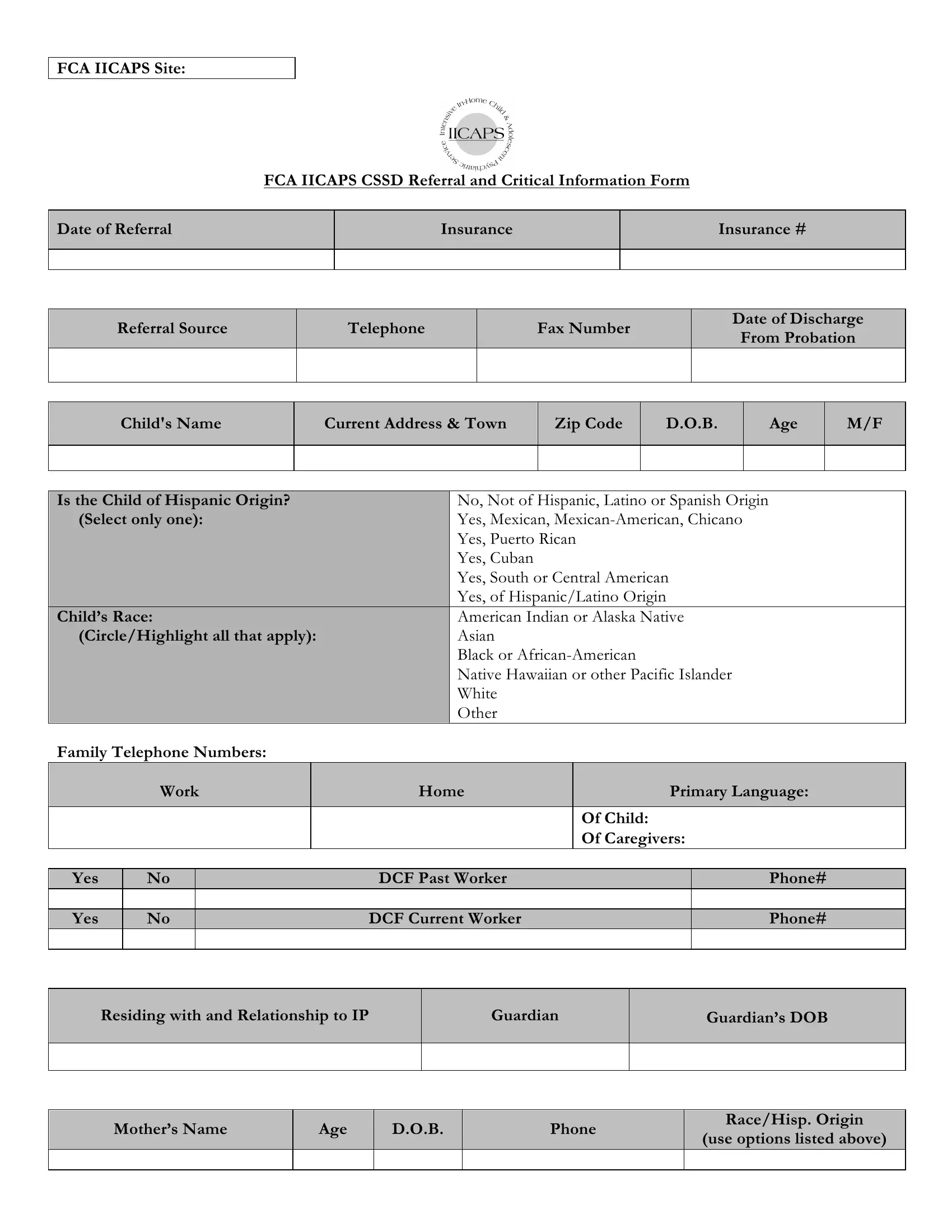
The IICAPS Referral Form is a crucial document designed to streamline the referral process to the Intensive In-home Child and Adolescent Psychiatric Services (IICAPS) program, a vital initiative for providing psychiatric services to children and adolescents within their home environment. Developed by the Family and Children's Aid (FCA) alongside the Yale Child Study Center, this comprehensive form captures all essential information required for a successful referral, including the child's personal information, insurance details, and the nature of their need for the service. Details such as the child’s name, current address, date of birth, gender, and ethnic origin are meticulously gathered to ensure a personalized care approach. Moreover, the form delves into the child's educational background, special education needs if any, and the family's language preferences, painting a holistic picture of the child's environment and support system. Intricate information regarding the child's behavioral concerns, family dynamics, and previous engagements with mental health services are also sought. Reflecting a holistic approach to care, the form prompts for details on the child's school performance, interactions within the educational setting, and the broader physical and social environment's impact on the child. Additionally, the form requests a thorough medical and psychiatric history to provide a comprehensive background for the IICAPS team. This detailed information aids the IICAPS coordinators in making informed decisions, ensuring that the child and family receive the most appropriate and effective services tailored to their unique situation.
| Question | Answer |
|---|---|
| Form Name | Iicaps Referral Form |
| Form Length | 4 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 1 min |
| Other names | FCA, IICAPS, FWSN, iicaps referral form |
FCA IICAPS Site:
FCA IICAPS CSSD Referral and Critical Information Form
Date of Referral |
Insurance |
Insurance # |
|
|
|
|
|
|
Referral Source
Telephone
Fax Number
Date of Discharge
From Probation
Child's Name
Current Address & Town
Zip Code
D.O.B.
Age
M/F
Is the Child of Hispanic Origin? |
|
No, Not of Hispanic, Latino or Spanish Origin |
||||||
(Select only one): |
|
Yes, Mexican, |
||||||
|
|
|
|
|
Yes, Puerto Rican |
|
|
|
|
|
|
|
|
Yes, Cuban |
|
|
|
|
|
|
|
|
Yes, South or Central American |
|
|
|
|
|
|
|
|
Yes, of Hispanic/Latino Origin |
|
|
|
Child’s Race: |
|
American Indian or Alaska Native |
||||||
(Circle/Highlight all that apply): |
|
Asian |
|
|
||||
|
|
|
|
|
Black or |
|
|
|
|
|
|
|
|
Native Hawaiian or other Pacific Islander |
|||
|
|
|
|
|
White |
|
|
|
|
|
|
|
|
Other |
|
|
|
Family Telephone Numbers: |
|
|
|
|
|
|||
|
Work |
|
Home |
|
Primary Language: |
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Of Child: |
|
|
|
|
|
|
|
|
Of Caregivers: |
||
|
|
|
|
|
|
|||
Yes |
No |
|
|
DCF Past Worker |
|
Phone# |
||
|
|
|
|
|
|
|||
Yes |
No |
|
|
DCF Current Worker |
|
Phone# |
||
|
|
|
|
|
|
|
|
|
Residing with and Relationship to IP
Guardian
Guardian’s DOB
Mother’s Name
Age
D.O.B.
Phone
Race/Hisp. Origin
(use options listed above)
Page 2 of 4 Child Name: _______________________________
Father’s Name
Age
D.O.B.
Phone
Race/Hisp. Origin
(use options listed above)
Child’s School
Grade
Special Ed.
Yes/No
School Contact
Other Household Members:
Name
Age
D.O.B.
Race/Hisp.
Origin
(use options listed above)
School
Relationship to
patient
Reason for Referral (box will expand on electronic format):
Behaviors of Concern:
Child Domain (topics might include presentation, behaviors, coping skills, cognitive abilities, etc):
Child/Family Domain (topics might include relationships within the family, parenting styles, history, crises management):
Child/School Domain(topics might include academic, behavioral, or social concerns):
Child/Physical Environment/Systems Domain (topics might include important service providers involved with the family, community support available, other systems’ involvement like DCF/CSSD):
What do you want IICAPS to work on with this child/family?:
Diagnosis (Include Codes):
♥ 2010 Yale Child Study Center. All materials are copyrighted and intended for IICAPS program use only. |
Rev. 8/9/10 |
Page 3 of 4
Child Name: _______________________________
I
II
III
IV
V CGAS
Current Medications:
Name
Dose
Frequency
Past Medications:
Name
Dose
Frequency
Past Psychiatric Hx: (include information about psychiatric hospitalizations (place of admission, dates, reason for admission) as well as other forms of mental health treatment provided to child.
CSSD Specific Information (can be captured in the referral narrative section within BMS):
•Case #:
•Targeted Class Member:
•Pending Charges:
Past Judicial Involvement (include FWSN, past charges, time in detention, etc):
Medical History (hospitalizations, medical conditions or concerns):
Current Treaters:
Family Member
Receiving Service
Institution/Agency
Type of Service
(individual therapy, inpatient, outpatient)
Telephone #
Name of Contact
♥ 2010 Yale Child Study Center. All materials are copyrighted and intended for IICAPS program use only. |
Rev. 8/9/10 |

Page 4 of 4
Child Name: _______________________________
Past Treaters:
Family Member Receiving Service
Institution/Agency
Type of Service
(individual therapy, inpatient, outpatient)
Telephone #
Name of Contact
IICAPS Coordinators are reminded to enter data into the IICAPS
♥ 2010 Yale Child Study Center. All materials are copyrighted and intended for IICAPS program use only. |
Rev. 8/9/10 |