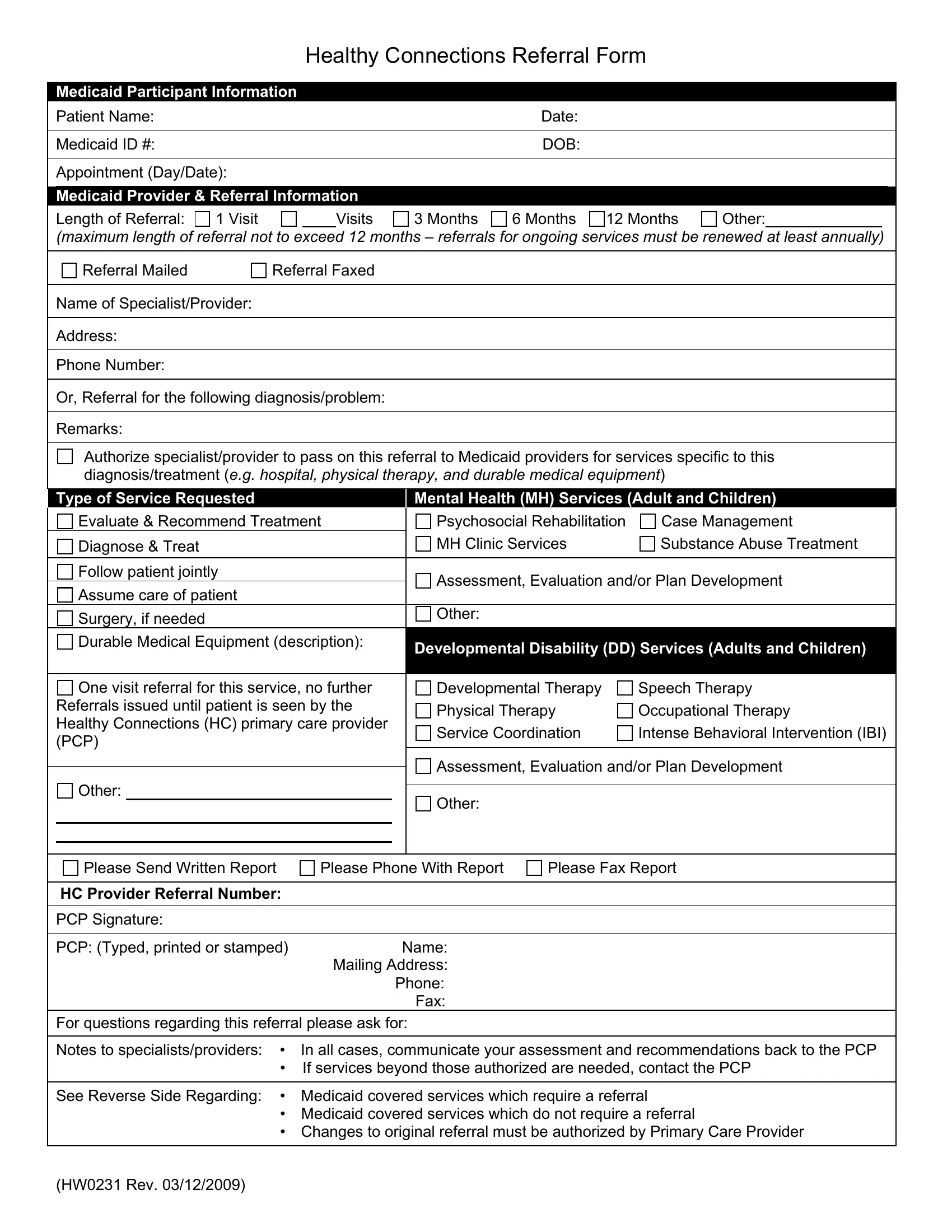
Ensuring timely and appropriate medical care for Medicaid participants is vital. The Healthy Connections Referral Form plays a crucial role in this process, bridging the gap between primary care providers (PCPs) and specialized medical services. This meticulously designed form captures essential Medicaid Participant Information, including the patient’s name, Medicaid ID, date of birth, and specifics about the appointment. It ventures further to encompass Medicaid Provider & Referral information, detailing the length of the referral—from a single visit up to a maximum of 12 months—and method of referral transmission, whether mailed or faxed. Important, too, is the inclusion of the specialist/provider's contact details and the type of service requested, which can range from mental health and substance abuse treatment to surgery and durable medical equipment needs. Notably, the form facilitates a streamlined communication line back to the PCP, mandating that specialists and providers share assessments and recommendations, vital for continuous patient care. For referrals surpassing the authorized services, re-initiating contact with the PCP is a procedural step indicated on the form. Additional components highlight services requiring a referral from the Healthy Connections PCP, contrasting with those services exempt from this requirement, illuminating the comprehensive nature of this instrumental form. Its strategic format and the detailed guidance it provides underscore its significance in the coordinated care ecosystem, ensuring Medicaid participants receive the necessary care, tailored to their specific health needs.
| Question | Answer |
|---|---|
| Form Name | Healthy Connections Referral Form |
| Form Length | 2 pages |
| Fillable? | Yes |
| Fillable fields | 59 |
| Avg. time to fill out | 12 min 22 sec |
| Other names | hw0231, healthy connections idaho, child and family connections referral form, children and family connection referral form |