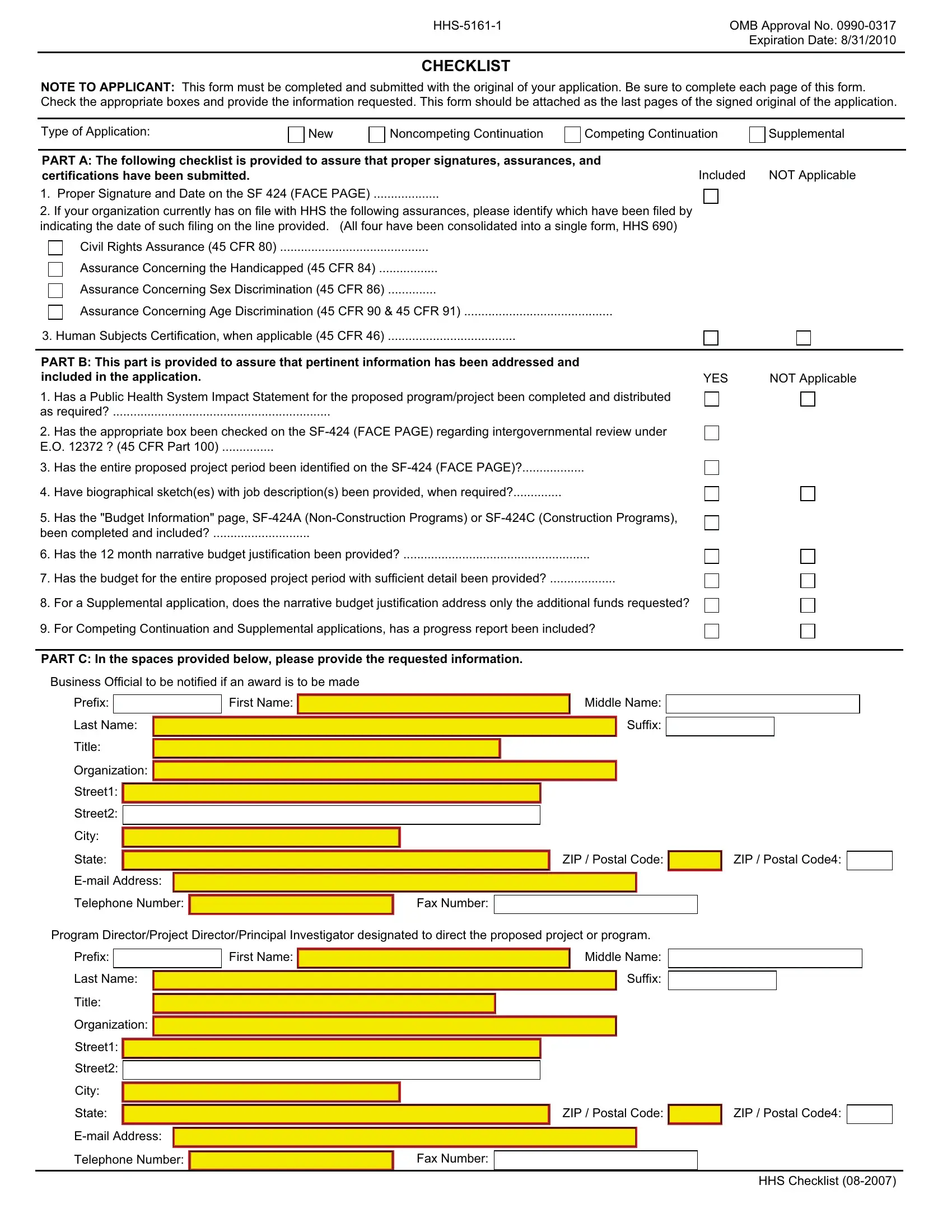
Navigating the intricacies of submitting applications within the health sector requires a thorough understanding of various forms and their significance, including the HHS-5161-1 form. This particular document is vital for those seeking approval for their applications from the U.S. Department of Health and Human Services (HHS). Marked by its OMB Approval No. 0990-0317, which signifies its clearance and standardization at a federal level, the form carries an expiration date, emphasizing the need for timely submission. It acts as a comprehensive checklist, guiding applicants through the necessary assurances, certifications, and particular information required to ensure a complete and compliant application submission. From securing proper signatures and dates on the SF 424 (Face Page) to providing detailed project narratives and financial justifications, the form spans a range of requirements that cover essential legal and procedural ground. Applicants are prompted to declare their adherence to regulations regarding civil rights, the welfare of the handicapped, sex and age discrimination, and other federal stipulations, reaffirming the importance of compliance and ethical standards in proposed projects. Furthermore, it addresses specifics such as the impact on public health systems, intergovernmental reviews under Executive Order 12372, and the inclusion of necessary biographical sketches for key project personnel. By ensuring each section of this form is accurately filled out and attached to an application, organizations can pave a clearer path towards achieving their goals under the auspices of HHS guidelines and support.
| Question | Answer |
|---|---|
| Form Name | Hhs 5161 1 Form |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | form 5161 form, form 5161 template, cfr hhs sf fill, hhs sf 1 fill |