In the complex and sensitive landscape of mental health care, ensuring patient privacy while facilitating necessary communication can be challenging. The Commonwealth of Massachusetts Department of Mental Health addresses this issue with the Authorization for Release of Information One-Way From Department of Mental Health form, commonly referred to as the HIPAA F-3 form. Designed with confidentiality in mind, this document empowers individuals to grant permission to the Department to share specific health information with designated persons, facilities, or agencies. Crucially, it delineates the types of information that can be shared, ranging from comprehensive medical records to more targeted data such as discharge summaries, treatment plans, and lab reports. Moreover, it underlines the conditional nature of this authorization, including the right to revoke consent at any time, the limitations of privacy once information is disclosed, and the voluntary basis of providing such authorization. This form demarcates a vital balance between maintaining confidentiality and enabling critical communications within the sphere of mental health services, demonstrating a nuanced approach to patient care and data protection.
| Question | Answer |
|---|---|
| Form Name | Hi Paa F 3 Form |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | how to massachusetts form release information, dmh release from form, massachusetts release information, dmh release way |
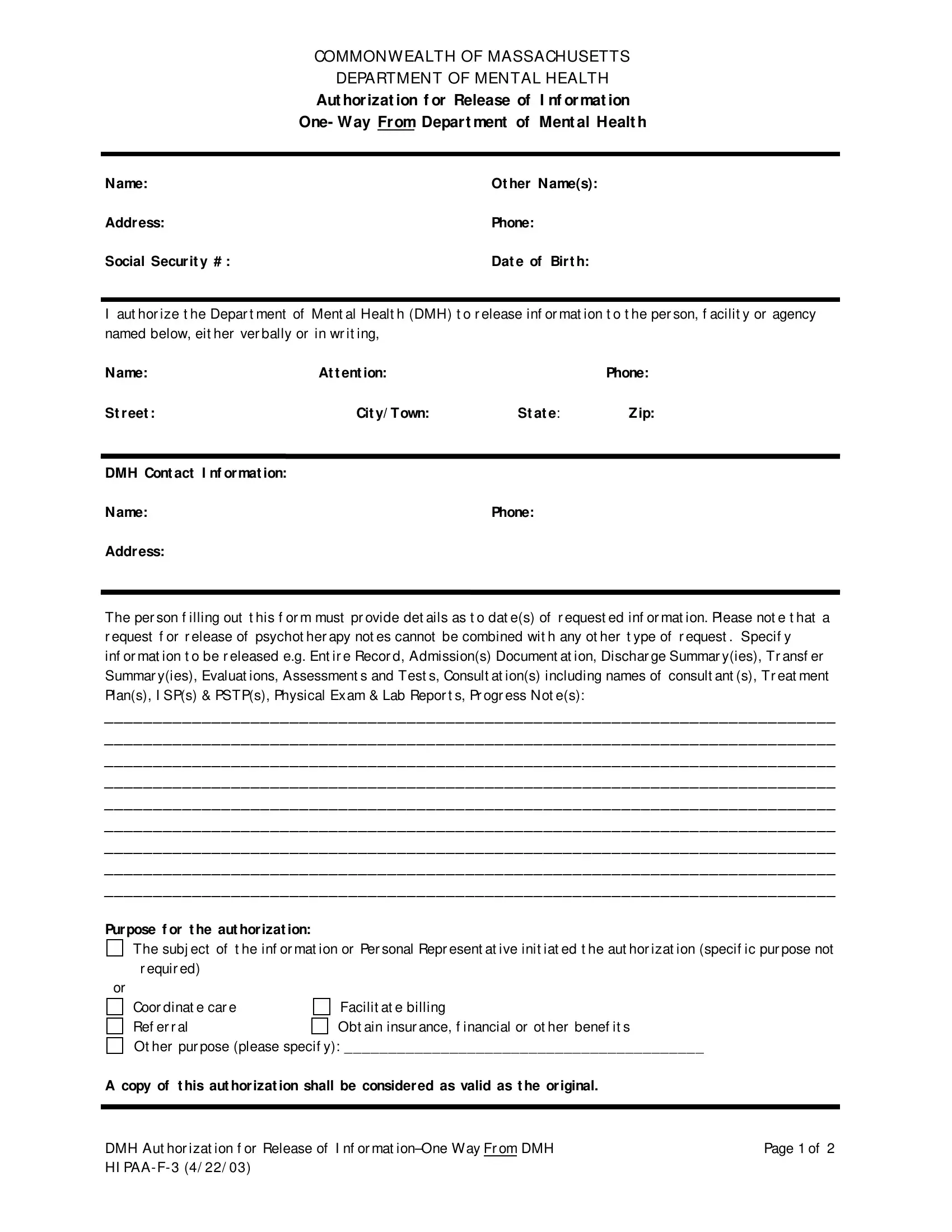
COMMONW EALTH OF MASSACHUSETTS
DEPARTMENT OF MENTAL HEALTH
Aut hor izat ion f or |
Release of |
I nf or mat ion |
One- W ay Fr om Depar t ment of |
Ment al Healt h |
|
|
|
|
|
|
|
N ame: |
Ot her N ame(s): |
|
Addr ess: |
Phone: |
|
Social Secur it y # : |
Dat e of Bir t h: |
|
Iaut hor ize t he Depar t ment of Ment al Healt h (DMH) t o r elease inf or mat ion t o t he per son, f acilit y or agency named below, eit her ver bally or in wr it ing,
N ame: |
At t ent ion: |
|
Phone: |
St r eet : |
Cit y/ T own: |
St at e: |
Zip: |
DMH Cont act |
I nf or mat ion: |
|
|
N ame: |
|
Phone: |
|
Addr ess: |
|
|
|
The per son f illing out t his f or m must pr ovide det ails as t o dat e(s) of r equest ed inf or mat ion. Please not e t hat a r equest f or r elease of psychot her apy not es cannot be combined wit h any ot her t ype of r equest . Specif y
inf or mat ion t o be r eleased e.g. Ent ir e Recor d, Admission(s) Document at ion, Dischar ge Summar y(ies), Tr ansf er Summar y(ies), Evaluat ions, Assessment s and Test s, Consult at ion(s) including names of consult ant (s), Tr eat ment Plan(s), I SP(s) & PSTP(s), Physical Exam & Lab Repor t s, Pr ogr ess Not e(s):
_ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _
_ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _
_ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _
_ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _
_ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _
_ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _
_ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _
_ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _
_ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _
Pur pose f or t he aut hor izat ion:
The subj ect of t he inf or mat ion or Per sonal Repr esent at ive init iat ed t he aut hor izat ion (specif ic pur pose not
r equir ed) |
|
|
or |
|
|
Coor dinat e car e |
Facilit at e billing |
|
Ref er r al |
Obt ain insur ance, f inancial or ot her benef it s |
|
Ot her pur pose (please specif y): _________________________________________ |
|
|
A copy of t his aut hor izat ion shall be consider ed as valid as t he or iginal. |
|
|
|
|
|
|
|
|
DMH Aut hor izat ion f or Release of I nf or mat |
Page 1 of 2 |
|
HI PAA- F- 3 (4/ 22/ 03) |
|
|
COMMONW EALTH OF MASSACHUSETTS
DEPARTMENT OF MENTAL HEALTH
Aut hor izat ion f or Release of I nf or mat ion (cont inued)
One- W ay Fr om Depar t ment of Ment al Healt h
N ame of per son/ f acilit y/ agency t hat DMH is t o r elease inf or mat ion t o: ___________________________
I under st and t hat I have a r ight t o r evoke t his aut hor izat ion at any t ime. I f I r evoke t his aut hor izat ion, I must do so in wr it ing and pr esent it t o DMH at t he DMH addr ess ident if ied on page one. I under st and t hat t he
r evocat ion will not apply t o inf or mat ion t hat has alr eady been r eleased pur suant t o t his aut hor izat ion. This aut hor izat ion will expir e in 12 mont hs unless ot her wise specif ied (specif y a dat e, t ime per iod or an
event ):________________________________ . I under st and t hat once t he above inf or mat ion is disclosed t o
a per son, f acilit y or agency out side DMH, t he r ecipient may r edisclose it and t he inf or mat ion may not be
pr ot ect ed by f eder al or st at e pr ivacy laws or r egulat ions. I under st and t hat aut hor izing t he use or disclosur e of t he inf or mat ion ident if ied above is volunt ar y. I need not sign t his f or m t o r eceive t r eat ment or ser vices
f r om DMH. However , lack of abilit y t o shar e or obt ain inf or mat ion may pr event DMH f r om pr oviding appr opr iat e and necessar y car e.
_______________________________________________ |
_________________ |
Your signat ur e or Per sonal Repr esent at ive’s signat ur e |
Dat e |
_______________________________________________
Pr int name of signer
THE FOLLOWI NG I NFORMATI ON I S NEEDED I F SI GNED BY A PERSON AL REPRESENTATI VE
Type of aut hor it y (e.g., cour t appoint ed, cust odial par ent ) ______________________________________
Specially Aut hor ized Releases of I nf or mat ion (please init ial all t hat apply)
____ To t he ext ent t hat my medical r ecor d cont ains inf or mat ion concer ning alcohol or dr ug t r eat ment t hat is
pr ot ect ed by Feder al Regulat ion 42 CFR, Par t 2, I specif ically aut hor ize r elease of such inf or mat ion.
____ To t he ext ent t hat my medical r ecor d cont ains inf or mat ion concer ning HI V ant ibody and ant igen t est ing
t hat is pr ot ect ed by MGL c.111 §70F, or an HI V/ AI DS diagnosis or t r eat ment , I specif ically aut hor ize disclosur e of such inf or mat ion.
_______________________________________ |
______________ |
Your signat ur e or Per sonal Repr esent at ive’s signat ur e |
Dat e |
I N ST RUCT I ON S:
1.This f or m must be complet ed in f ull t o be consider ed valid.
2. Dist r ibut ion of copies: or iginal t o appr opr iat e DMH r ecor d; copy t o individual or Per sonal Repr esent at ive.
DMH For m Aut hor izat ion f or Release of I nf or mat ion- One Way Fr om DMH |
Page 2 of 2 |
HI PAA- F- 3 (4/ 22/ 03) |
|