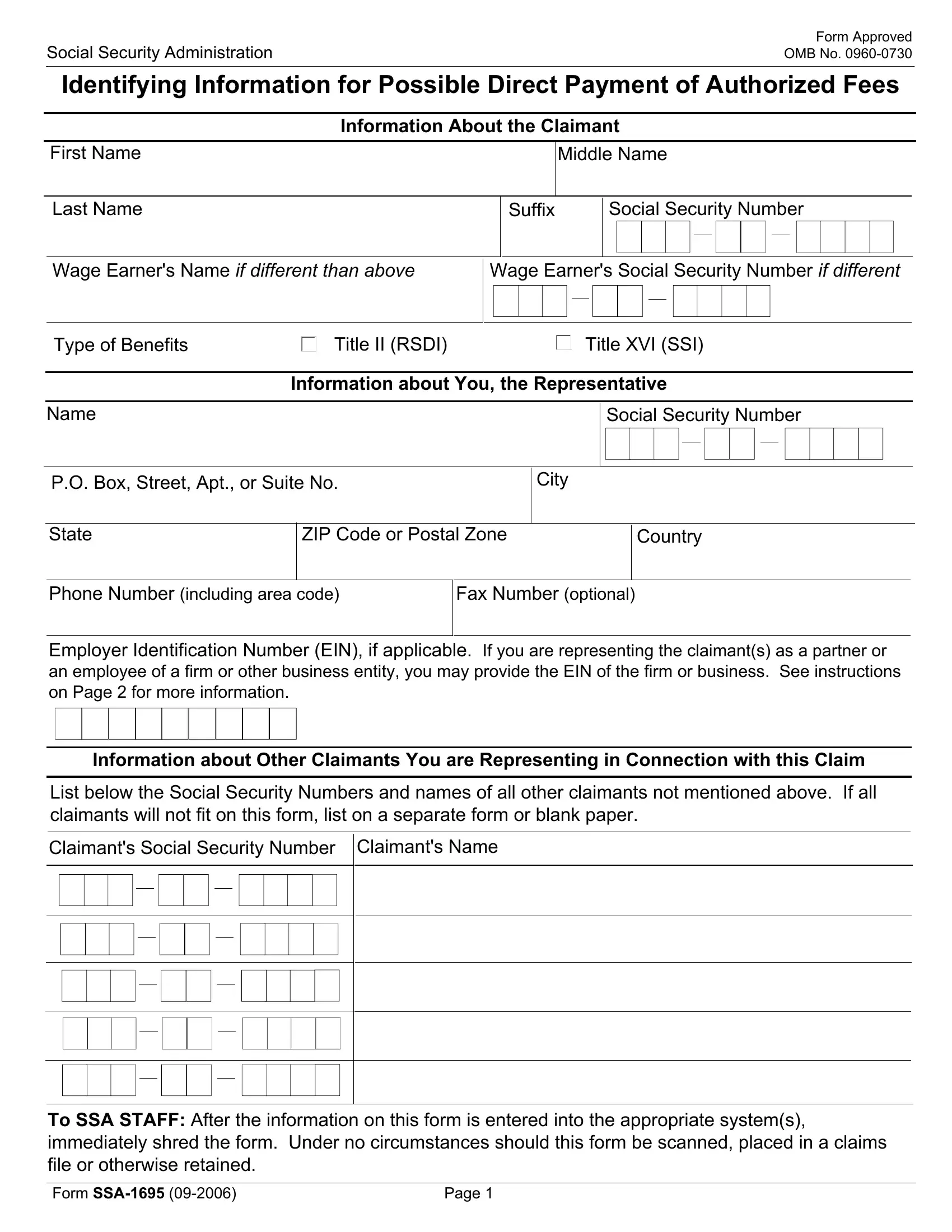
The Social Security Administration (SSA) Form SSA-1695, titled Identifying Information for Possible Direct Payment of Authorized Fees, serves a critical purpose for individuals who provide representation to claimants in Social Security matters. It is specifically designed for attorneys or representatives who wish to receive direct payment from the SSA for authorized fees, streamlining the process by which these payments are made and ensuring adherence to legal and procedural requirements. At its core, the form collects detailed identifying information about the claimant, the representative, and, if applicable, other claimants being represented in the same matter. This includes names, Social Security numbers (SSNs), addresses, and types of benefits being claimed. The form also facilitates the correct attribution of payments to representatives, possibly via direct deposit, and helps the SSA meet its reporting obligations, notably the issuance of Form 1099-MISC for tax purposes. Completing Form SSA-1699 is a prerequisite for providing the necessary information for these transactions. Moreover, personal details like changes in name due to marriage can also affect how Social Security records are updated, meriting special attention when filling out the form. Failure to provide complete and accurate information may result in nonpayment of services provided to the claimant, highlighting the form's importance in the process of legal representation before the SSA. Additionally, it fulfills crucial privacy and legal compliance roles, with its use regulated under specific Social Security Acts. This thorough procedural requirement underscores the balance between facilitating authorized fee payments and maintaining rigorous privacy standards.
| Question | Answer |
|---|---|
| Form Name | Form Ssa 1695 |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | G SSA 1695 1 identifying information for possible direct payment of authorized fees |