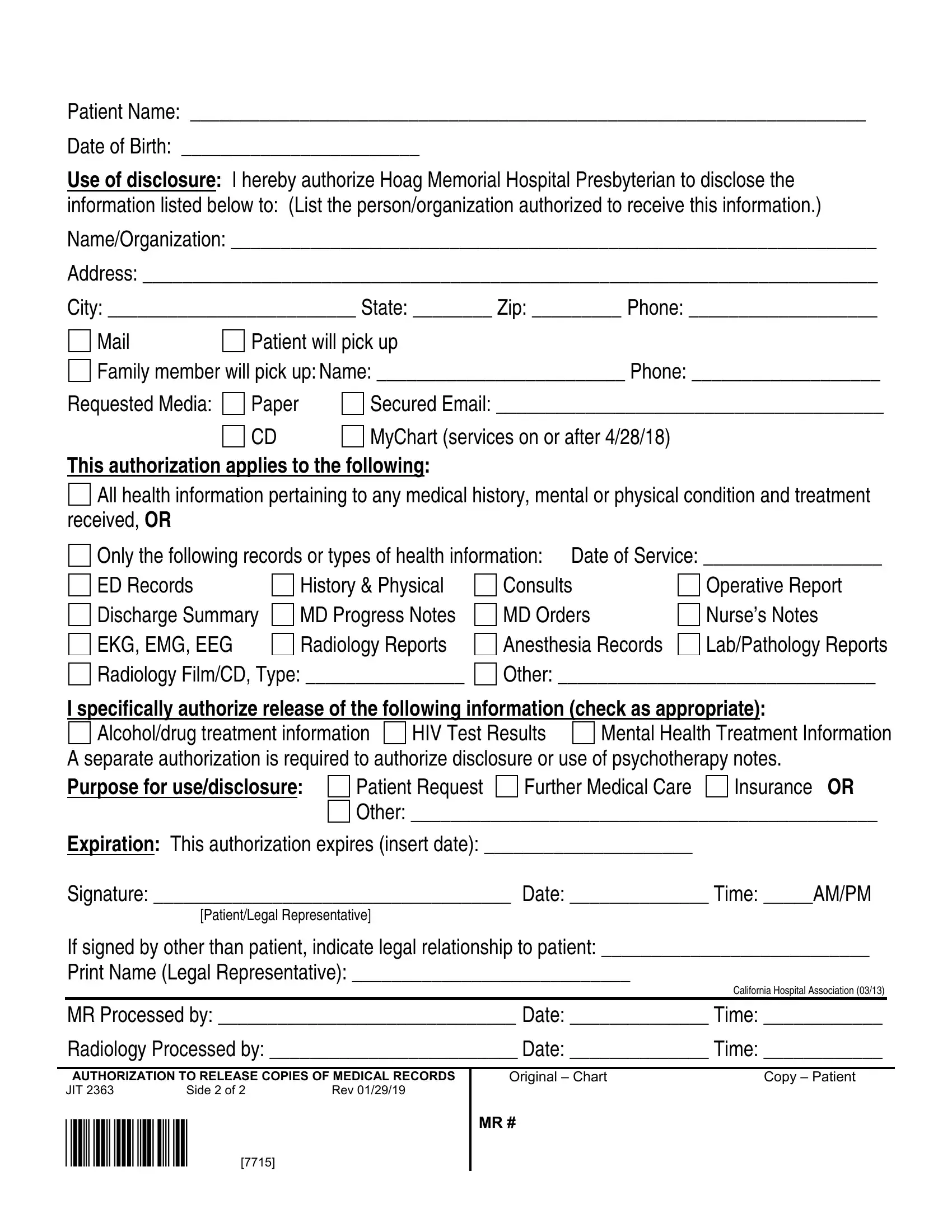
In today's healthcare landscape, the Hoag Medical Records form stands as a crucial document designed to facilitate the safe and regulated sharing of patient information among medical professionals, patients, and authorized third parties. This form, meticulously crafted by Hoag Memorial Hospital Presbyterian, serves multiple purposes, including but not limited to, enabling patients to request their medical records in various formats (such as paper, CD, or via secured email) and specifying the type of health information to be disclosed. Whether for continued medical care, insurance purposes, or personal records, patients have the flexibility to limit the disclosure to comprehensive health information or specific types of records such as lab reports, radiology reports, or mental health treatment details. Importantly, the form not only outlines the process for obtaining these records but also enshrines patient rights regarding the authorization of such disclosures. Essentially, by completing this document, patients authorize Hoag Memorial Hospital Presbyterian to release their medical information in accordance with California and Federal privacy laws, while also retaining the ability to revoke this authorization at any time. The thoughtful inclusion of protections against unauthorized re-disclosure underscores the form's role in safeguarding patient privacy, thereby embodying the delicate balance between the need for information sharing in healthcare and the imperative of protecting individual privacy.
| Question | Answer |
|---|---|
| Form Name | Hoag Medical Records Form |
| Form Length | 2 pages |
| Fillable? | Yes |
| Fillable fields | 56 |
| Avg. time to fill out | 11 min 46 sec |
| Other names | hoag medical records fax, hoag release medical records, mychart hoag, hoag records |
Patient Name: ____________________________________________________________________
Date of Birth: ________________________
Use of disclosure: I hereby authorize Hoag Memorial Hospital Presbyterian to disclose the
information listed below to: (List the person/organization authorized to receive this information.)
Name/Organization: _________________________________________________________________
Address: __________________________________________________________________________
City: _________________________ State: ________ Zip: _________ Phone: ___________________
|
Patient will pick up |
Family member will pick up: Name: _________________________ Phone: ___________________
Requested Media: |
Paper |
Secured Email: _______________________________________ |
|
CD |
MyChart (services on or after 4/28/18) |
This authorization applies to the following:
All health information pertaining to any medical history, mental or physical condition and treatment received, OR
Only the following records or types of health information: Date of Service: __________________
ED Records |
History & Physical |
Consults |
Operative Report |
Discharge Summary |
MD Progress Notes |
MD Orders |
Nurse’s Notes |
EKG, EMG, EEG |
Radiology Reports |
Anesthesia Records |
Lab/Pathology Reports |
Radiology Film/CD, Type: ________________ |
Other: ________________________________ |
||
I specifically authorize release of the following information (check as appropriate):
Alcohol/drug treatment information HIV Test Results Mental Health Treatment Information A separate authorization is required to authorize disclosure or use of psychotherapy notes.
Purpose for use/disclosure:
Patient Request |
Further Medical Care |
Insurance OR |
Other: _______________________________________________
Expiration: This authorization expires (insert date): _____________________
Signature: ____________________________________ Date: ______________ Time: _____AM/PM
[Patient/Legal Representative]
If signed by other than patient, indicate legal relationship to patient: ___________________________
Print Name (Legal Representative): ____________________________
California Hospital Association (03/13)
MR Processed by: ______________________________ Date: ______________ Time: ____________
Radiology Processed by: _________________________ Date: ______________ Time: ____________
AUTHORIZATION TO RELEASE COPIES OF MEDICAL RECORDS
JIT 2363 |
Side 2 of 2 |
Rev 01/29/19 |
*7715* [7715]
Original – Chart |
Copy – Patient |
MR #
AUTHORIZATION TO RELEASE COPIES OF MEDICAL RECORDS
Hoag Memorial Hospital Presbyterian
Dear Patient:
Completion of this document authorizes the disclosure and/or use of individually identifiable health information, as set forth below, consistent with California and Federal law concerning the privacy of such information. Failure to provide all information requested may invalidate this authorization:
Notice of Rights and Other Information:
I may refuse to sign this authorization. My refusal will not affect my ability to obtain treatment or payment or eligibility for benefits.
I may revoke this authorization at any time. My revocation must be in writing, signed by me or on my behalf, and delivered to Hoag Hospital, Health Information Department, One Hoag Drive, Newport Beach, CA 92658. My revocation will be effective upon receipt, but will not be effective to the extent that the requestor or others have acted in reliance on this authorization.
I have a right to receive a copy of this authorization.
Information disclosed pursuant to this authorization could be
I may inspect or obtain a copy of the health information that I am being asked to use or disclose.
Complete request information on reverse side... |
Side 1 of 2 |
*7715* [7715]