
Once you open the online editor for PDFs by FormsPal, it is possible to fill out or alter decision unpaid pdf here. To make our tool better and more convenient to utilize, we consistently come up with new features, taking into account feedback from our users. With a few basic steps, you may begin your PDF editing:
Step 1: Simply click the "Get Form Button" in the top section of this site to start up our form editor. This way, you will find everything that is required to fill out your document.
Step 2: With our online PDF tool, you're able to accomplish more than just fill in blank form fields. Edit away and make your docs appear great with customized textual content incorporated, or fine-tune the file's original content to excellence - all comes along with an ability to add just about any photos and sign the file off.
As a way to fill out this form, be certain to enter the necessary information in every single blank:
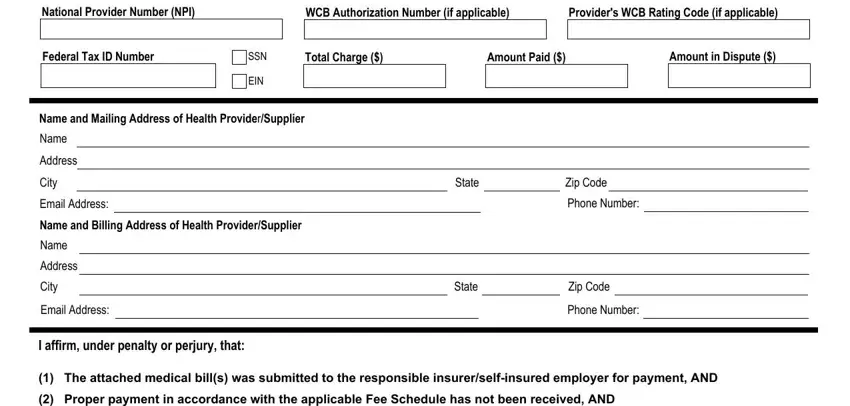
1. It's important to fill out the decision unpaid pdf accurately, therefore take care when filling out the areas containing all these blanks:
2. Once your current task is complete, take the next step – fill out all of these fields - RETURN THIS COMPLETED AND SIGNED with their corresponding information. Make sure to double check that everything has been entered correctly before continuing!

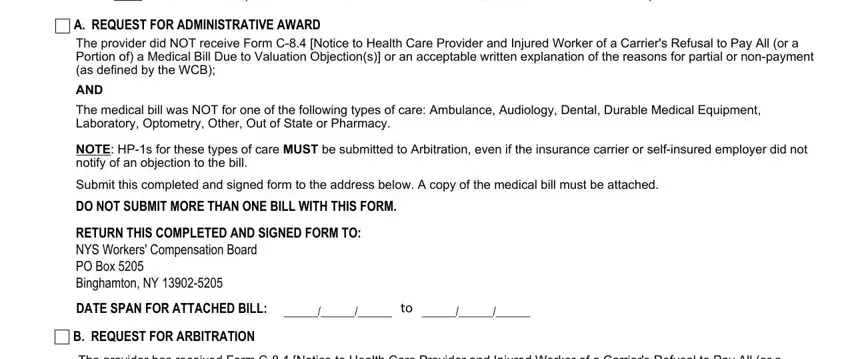
3. This next step focuses on WCB Case Number, Name of Injured Worker First Name, Injured Workers Social Security, Date of InjuryIllness, Insurer or SelfInsured Employer ID, Claim Administrator Claim Number, Name of Employer, Name and Mailing Address of Insurer, Name, Address, City, CHECK APPLICABLE TYPE OF CARE, State, Zip Code, and Acupuncturist - fill out all of these fields.
It's simple to make errors while filling in your Acupuncturist, for that reason make sure to look again before you'll submit it.
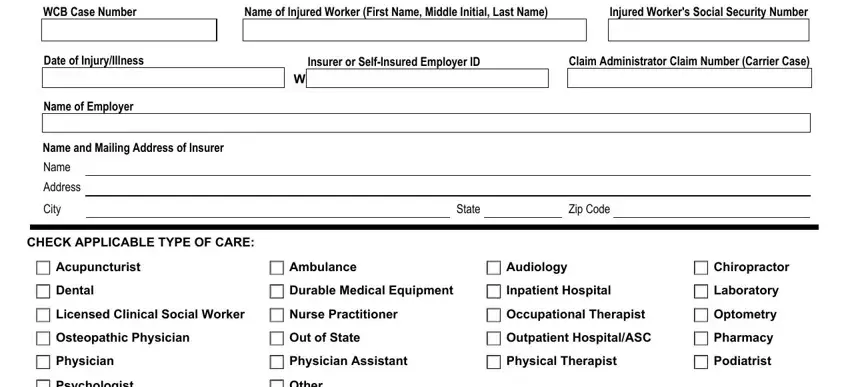
4. This next section requires some additional information. Ensure you complete all the necessary fields - National Provider Number NPI, WCB Authorization Number if, Providers WCB Rating Code if, Federal Tax ID Number, SSN, EIN, Name and Mailing Address of Health, Name, Address, City, Email Address, Name and Billing Address of Health, Name, Address, and City - to proceed further in your process!
5. And finally, the following final subsection is what you will need to finish before closing the PDF. The fields at this point are the next: I will abide by the WCBs decision, Health ProviderSuppliers Signature, Date, ANY PERSON WHO KNOWINGLY AND WITH, and Any questions regarding the.
Step 3: Always make sure that the information is accurate and then press "Done" to finish the project. Right after getting afree trial account with us, it will be possible to download decision unpaid pdf or send it via email right away. The form will also be at your disposal through your personal account page with all of your edits. We don't sell or share any details you provide when working with documents at FormsPal.