
Any time you wish to fill out HSA, you won't have to download any applications - just use our online PDF editor. To make our tool better and simpler to utilize, we continuously come up with new features, taking into account suggestions from our users. Starting is easy! All you have to do is take these easy steps down below:
Step 1: Press the "Get Form" button above. It's going to open our pdf tool so you can start completing your form.
Step 2: When you open the tool, there'll be the form made ready to be filled out. In addition to filling out various blank fields, you could also do other sorts of actions with the Document, specifically adding any text, modifying the initial textual content, adding illustrations or photos, affixing your signature to the PDF, and more.
This PDF doc will involve specific information; to ensure consistency, you should take note of the recommendations listed below:
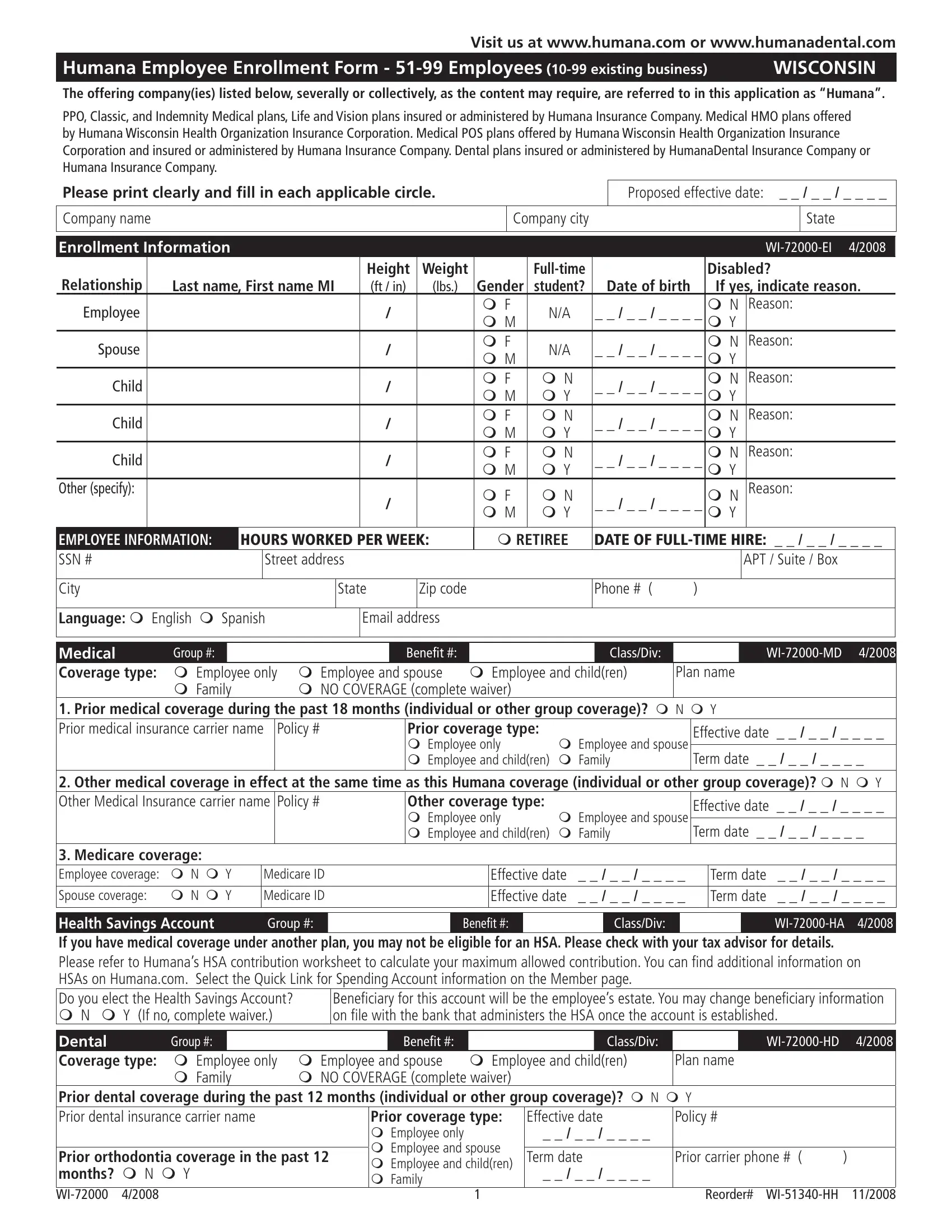
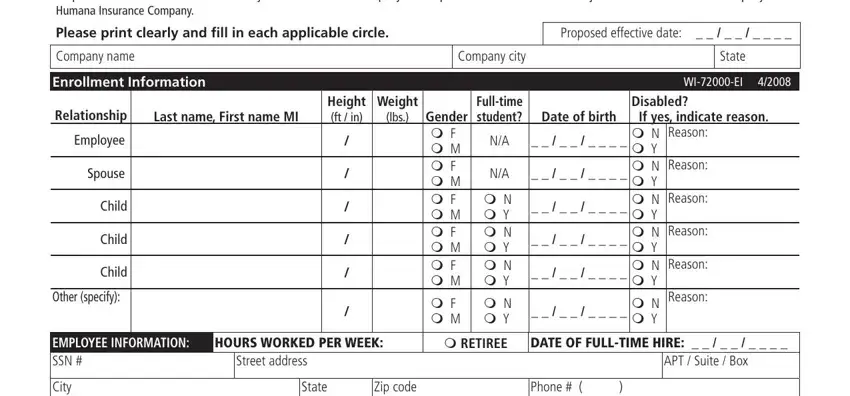
1. You will want to complete the HSA accurately, so be attentive while filling in the parts that contain all of these fields:
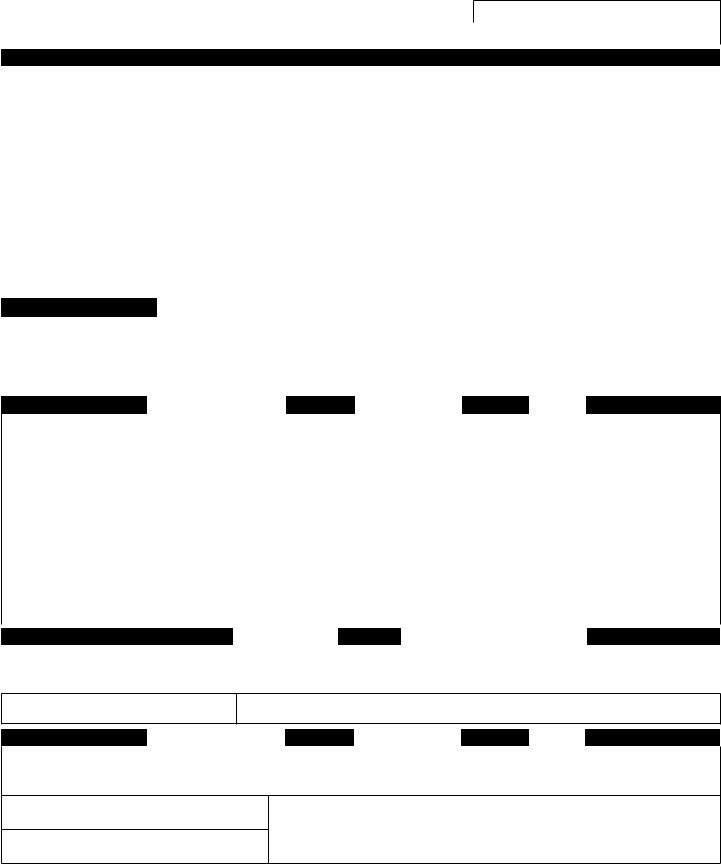
2. Given that the last section is completed, you're ready to insert the needed specifics in Language m English m Spanish, Email address, Group, Medical Coverage type m Employee, m NO COVERAGE complete waiver, m Family, ClassDiv, Benefit, Plan name, WIMD, Prior coverage type m Employee, m Employee and spouse, Effective date, Term date, and Other medical coverage in effect so you're able to progress to the 3rd step.
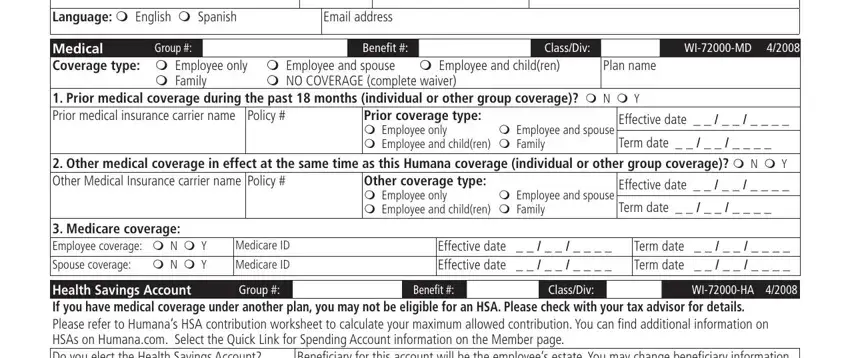
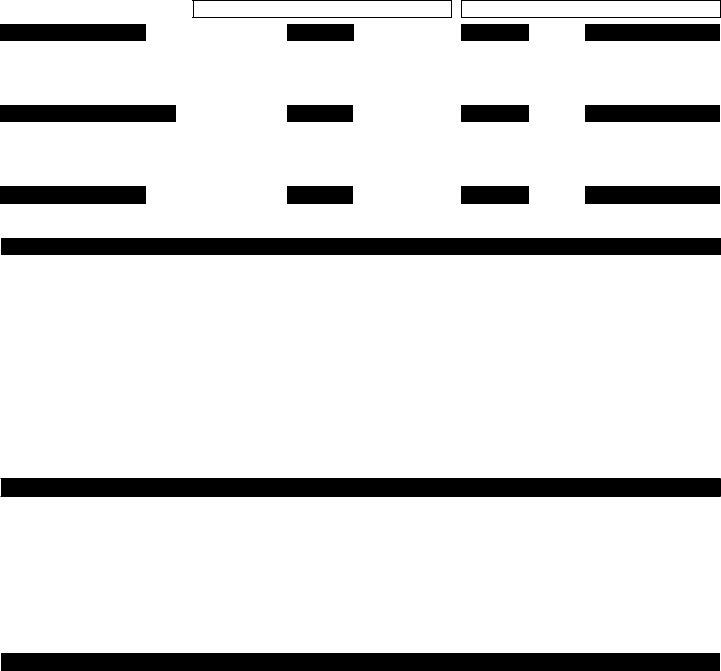
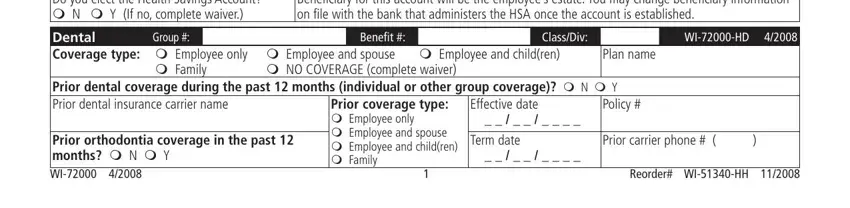
3. This 3rd part is considered relatively straightforward, Health Savings Account If you have, Beneficiary for this account will, Group, Dental Coverage type m Employee, m NO COVERAGE complete waiver, m Family, ClassDiv, Benefit, Policy, Plan name, WIHD, Prior orthodontia coverage in the, Prior coverage type m Employee, Effective date Term date, and Prior carrier phone - all these fields has to be completed here.
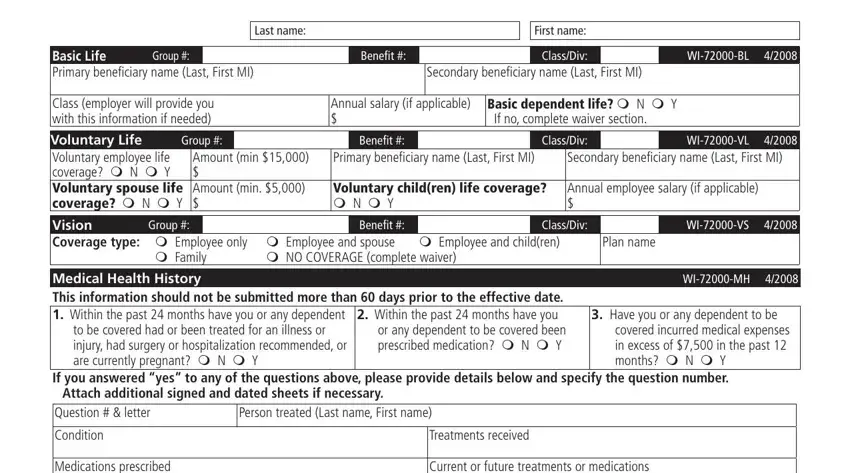
4. To go onward, the next stage involves filling in a couple of form blanks. These comprise of Basic Life Primary beneficiary, Group, Benefit, Last name, First name, ClassDiv, WIBL, Secondary beneficiary name Last, Class employer will provide you, Annual salary if applicable, Basic dependent life m N m Y If no, Group, Voluntary Life Voluntary employee, Amount min Amount min, and Benefit, which are essential to moving forward with this particular form.
People frequently make mistakes when filling in Voluntary Life Voluntary employee in this area. You should definitely revise whatever you enter right here.
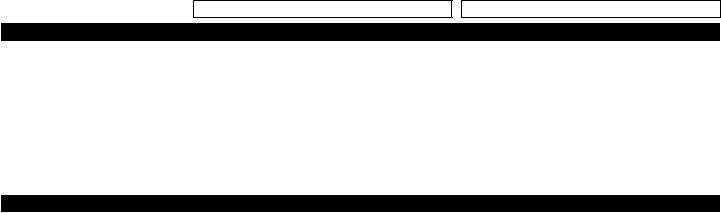
5. Since you get close to the end of the file, there are several more things to complete. In particular, Medications prescribed, Current or future treatments or, Date diagnosed, Date last seen by a doctor, Waiver refusal of coverage I, m Spousal coverage m Medicare, I decline to apply for group, WIWV, WIAA, Agreement True and complete, and I have read this document or it must be filled in.
Step 3: When you've reviewed the details you filled in, press "Done" to conclude your form at FormsPal. Go for a free trial plan with us and gain immediate access to HSA - download, email, or edit in your personal cabinet. At FormsPal.com, we strive to make sure all your information is maintained secure.