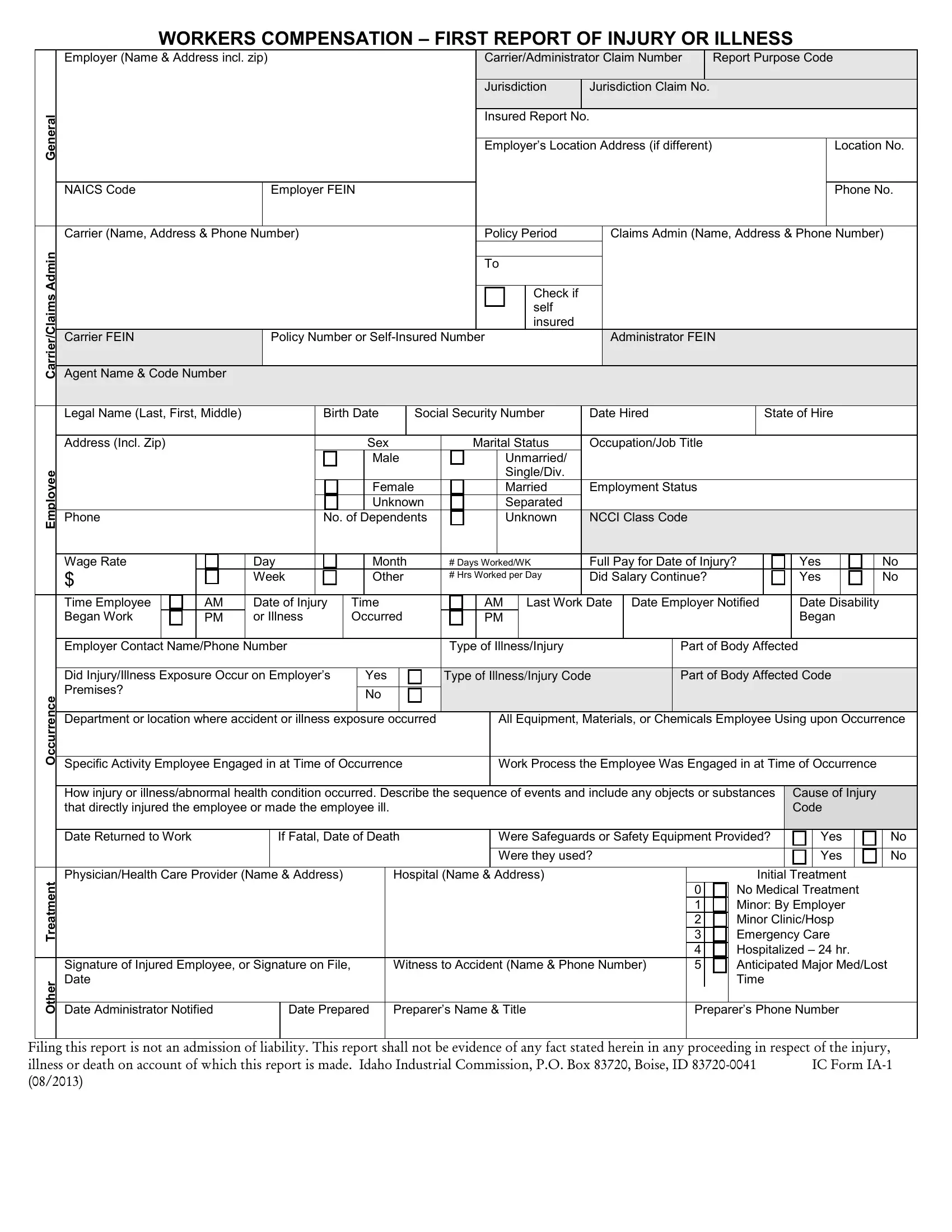
Navigating through the intricacies of worker's compensation can be daunting, especially when it involves documenting an injury or illness. At the heart of this process is the Ic Ia 1 form, a critical document designed to record the initial details concerning workplace incidents leading to injuries or illnesses. This form serves as the first report of injury or illness, requiring comprehensive information such as employer details, insurance carrier information, and specifics about the employee involved, including their job title, nature of the injury or illness, and circumstances surrounding the event. It is meticulously structured to capture data ranging from the date of injury, whether the injury occurred on the employer's premises, to specifics about the injury or illness itself, including the part of the body affected and the type of illness or injury code. Additionally, it inquires about the use of safety equipment, details of the treatment provided, and the administrative aspects of filing and notification, underlining the importance of accurate and prompt reporting. Employers and claims administrators must approach this form with diligence, as it sets the stage for the claims process, aids in the investigation, and ensures compliance with jurisdictional requirements. Importantly, the meticulous completion of this form underscores an essential aspect of workplace safety and workers' compensation procedures, facilitating a streamlined process for all parties involved. Furthermore, it’s noteworthy that the act of filing this report is not an admission of liability by the employer, nor will the contents necessarily serve as evidence in any related proceedings, providing a level of protection for the information provided. The Ic Ia 1 form is an indispensable element of the workers' compensation ecosystem, paving the way for a systematic approach to handling workplace injuries and illnesses.
| Question | Answer |
|---|---|
| Form Name | Ic Form Ia 1 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | ic_1_froi first report of injury idaho illinois iowa form |
WORKERS COMPENSATION – FIRST REPORT OF INJURY OR ILLNESS
|
|
Employer (Name & Address incl. zip) |
|
|
|
|
|
|
|
|
|
|
|
Carrier/Administrator Claim Number |
|
Report Purpose Code |
|
|
||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Jurisdiction |
|
Jurisdiction Claim No. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
General |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Insured Report No. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Employer’s Location Address (if different) |
|
|
|
|
|
|
|
Location No. |
|
|||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
NAICS Code |
|
|
|
|
|
Employer FEIN |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Phone No. |
|
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
Carrier (Name, Address & Phone Number) |
|
|
|
|
|
|
|
|
|
|
|
Policy Period |
|
|
|
Claims Admin (Name, Address & Phone Number) |
|
|||||||||||||||||||||||||||||||||||
Admin |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
To |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Carrier/Claims |
|
Agent Name & Code Number |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Check if |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
self |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
insured |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Carrier FEIN |
|
|
|
|
|
Policy Number or |
|
|
|
|
|
|
Administrator FEIN |
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
Legal Name (Last, First, Middle) |
|
|
|
|
Birth Date |
|
Social Security Number |
|
Date Hired |
|
|
State of Hire |
|
|
||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
Address (Incl. Zip) |
|
|
|
|
|
|
|
|
|
|
|
Sex |
|
|
|
Marital Status |
|
Occupation/Job Title |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Male |
|
|
|
|
|
|
|
|
Unmarried/ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
Employee |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Single/Div. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Female |
|
|
|
|
|
|
|
|
Married |
|
Employment Status |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Unknown |
|
|
|
|
|
|
|
Separated |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
Phone |
|
|
|
|
|
|
|
No. of Dependents |
|
|
|
|
|
|
|
Unknown |
|
NCCI Class Code |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
Wage Rate |
|
|
|
Day |
|
|
|
|
|
Month |
|
|
# Days Worked/WK |
|
Full Pay for Date of Injury? |
|
|
|
Yes |
|
|
|
|
|
|
No |
|
|||||||||||||||||||||||||
|
$ |
|
|
|
|
|
|
Week |
|
|
|
|
|
Other |
|
|
# Hrs Worked per Day |
|
Did Salary Continue? |
|
|
|
|
|
Yes |
|
|
|
|
|
|
No |
|
|||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
Time Employee |
|
|
|
AM |
Date of Injury |
|
Time |
|
|
|
|
|
AM |
|
|
Last Work Date |
Date Employer Notified |
|
Date Disability |
|
|
|||||||||||||||||||||||||||||||
|
|
Began Work |
|
|
|
PM |
or Illness |
|
Occurred |
|
|
|
|
|
PM |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Began |
|
|
||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Employer Contact Name/Phone Number |
|
|
|
|
|
|
|
|
Type of Illness/Injury |
|
|
|
|
|
|
Part of Body Affected |
|
|
||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||
|
|
Did Injury/Illness Exposure Occur on Employer’s |
|
|
|
Yes |
|
|
|
TypeofIllness/InjuryCode |
|
|
Part of Body Affected Code |
|
|
|||||||||||||||||||||||||||||||||||||||
|
|
Premises? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
Occurrence |
|
|
|
|
|
|
|
|
|
|
|
|
No |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Department or location where accident or illness exposure occurred |
|
|
|
|
|
|
All Equipment, Materials, or Chemicals Employee Using upon Occurrence |
|
|||||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||
|
|
Specific Activity Employee Engaged in at Time of Occurrence |
|
|
|
|
|
|
|
Work Process the Employee Was Engaged in at Time of Occurrence |
|
|
||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||
|
|
How injury or illness/abnormal health condition occurred. Describe the sequence of events and include any objects or substances |
|
Cause of Injury |
|
|
||||||||||||||||||||||||||||||||||||||||||||||||
|
|
that directly injured the employee or made the employee ill. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Code |
|
|
|||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Date Returned to Work |
|
|
|
|
|
If Fatal, Date of Death |
|
|
|
|
|
|
|
Were Safeguards or Safety Equipment Provided? |
|
|
Yes |
|
|
|
No |
|
||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Were they used? |
|
|
|
|
|
|
|
|
|
|
Yes |
|
|
|
No |
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Treatment |
Physician/Health Care Provider (Name & Address) |
Hospital (Name & Address) |
3 |
Initial Treatment |
|
|
|
|
Emergency Care |
||
|
|
|
|
0 |
No Medical Treatment |
|
|
|
|
1 |
Minor: By Employer |
|
|
|
|
2 |
Minor Clinic/Hosp |
|
|
|
|
4 |
Hospitalized – 24 hr. |
|
Signature of Injured Employee, or Signature on File, |
Witness to Accident (Name & Phone Number) |
5 |
Anticipated Major Med/Lost |
|
Other |
Date |
|
|
|
Time |
Date Administrator Notified |
Date Prepared |
Preparer’s Name & Title |
Preparer’s Phone Number |
||
Filing this report is not an admission of liability. This report shall not be evidence of any fact stated herein in any proceeding in respect of the injury,
illness or death on account of which this report is made. Idaho Industrial Commission, P.O. Box 83720, Boise, ID