The Illinois DNR Form is an agreement between patient and physician about the necessity of resuscitation procedures when a patient has a heart or breath attack. It is a common form for people who consider any resuscitation operations such as CPR or others useless for their state. Usually, people decide to sign the Do Not Resuscitate (DNR) Form when their state is terminal, or they have a chronic, incurable disease.
One of the main requirements of this form is a physician’s signature, as they should agree on the implementation of this paper. If the physician refuses to sign the DNR form, it will not be valid. However, if both the patient and the physician agree on this decision, all medical staff will not take any resuscitation operations for the patient.
Build Your Document
Answer a few simple questions to make your document in minutes
Save and Print
Save progress and finish on any device, download and print anytime
Sign and Use
Your valid, lawyer-approved document is ready
According to Illinois laws, three people should sign the form to make it valid: patient, physician, witness. Any person over 18 years old can become a witness in the signing procedure regardless of the relation of this person to the patient.
Regarding requirements to the patient’s state, this person should be able to decide about signing the Illinois DNR form individually. If the health condition does not allow the patient to be conscious, representatives of this person can act on their behalf. Nevertheless, the representative should have the right to participate in the decision-making process, so the person has to be an attorney-in-law or guardian of the patient.
The state introduced some changes to laws regulating the application of DNR forms recently. Nowadays, there is another form that helps to control and manage the life-sustaining processes, including resuscitation ones—POLST. POLST (Practitioner Orders for Life-Sustaining Treatment) is a comprehensive form that is accepted by a bigger number of medical organizations than the DNR form. The POLST form is regulated by statute 755 ILCS 40/65 of the Illinois Compiled Statutes, and it sets requirements for completion of the form.
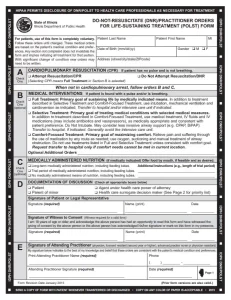
When a patient is sure about the completion of the Illinois DNR form, they can easily fill it out without the help of attorneys. Follow the tutorial presented below to complete all the fields of the form correctly.
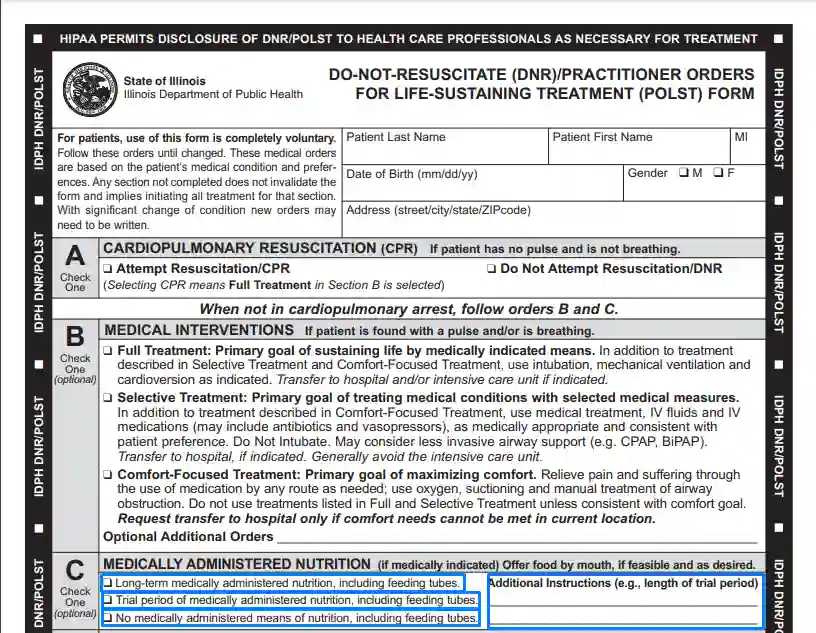
1. Enter Personal Data About Patient
The first part of the DNR/POLST form requires important information about voluntary participation in this procedure. It is recommended that the patient reads it carefully before filling out the form. If the patient is sure about the decision, they should enter the full name, date of birth, sex, and address into the first lines of the form.
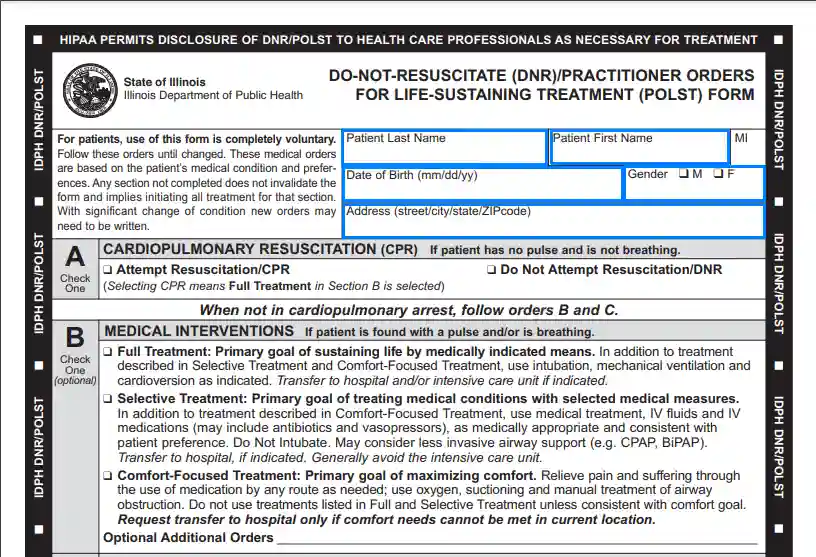
2. Choose Preferable Option About CPR
Patients should express opinions about the implementation of CPR actions in case of breath or heart failure. Select a suitable option and put a checkmark in the box there.
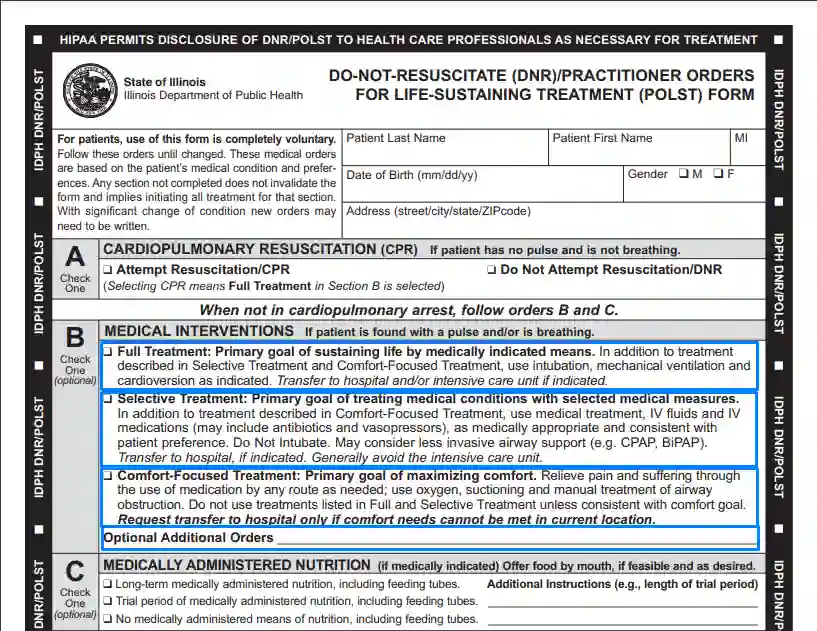
3. Select the Type of Treatment
In part B, the patient has to select the level of comprehensiveness of the treatment applied to them.
There are three options patients can choose from:
The difference between these alternatives is described in the form. So, choose the one you want to be applied to you in such a situation when you still have a pulse and are breathing. If there is no suitable option for you, you can write in your approach to treatment.
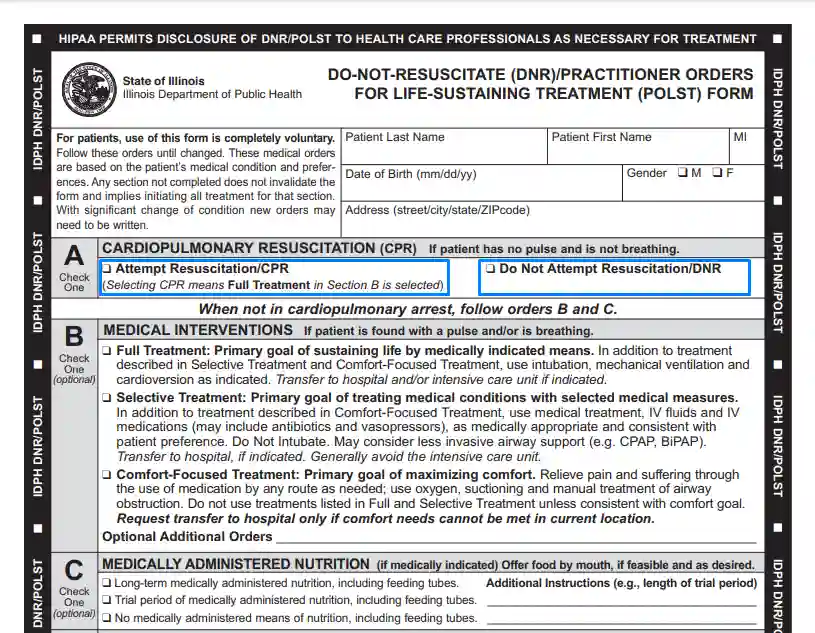
4. Choose the Means of Nutrition
There are situations when patients cannot feed themselves, and in this case, they need to choose the preferable option of nutrition provided by medical staff. The variants differ in the length of the provided nutrition period. However, if you want to offer your length of nutrition period, you can enter it in an additional box.
5. Determine the Person Filling Out the Form
In the first lines of part D, you should select a checkbox based on who is filling out the form. So, here you should declare if you are the patient or representative of the treated person.
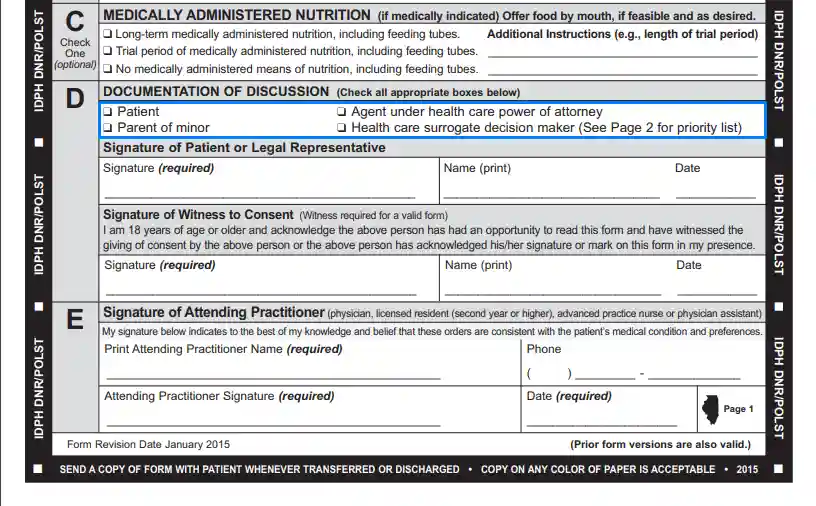
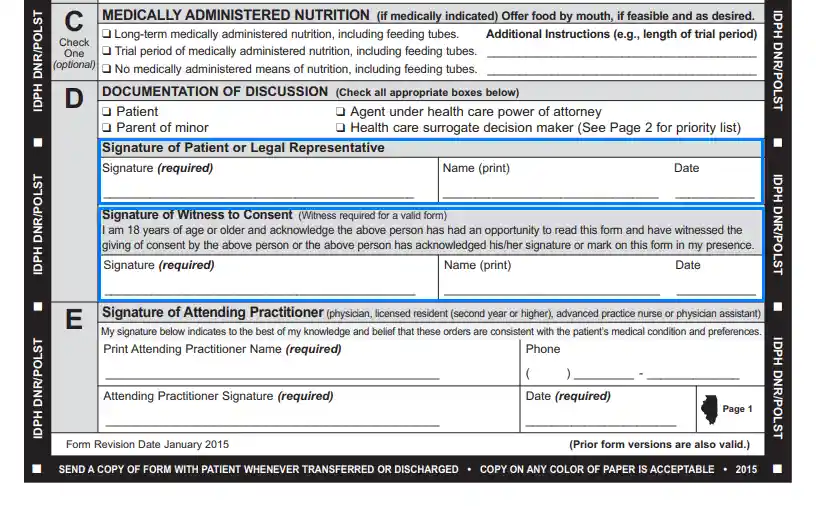
6. Sign DNR Form
Enter your signature, full name, and the date of the completion process. A witness should confirm the accuracy of filling out the form in the same part with a signature, full name, and date of witnessing.
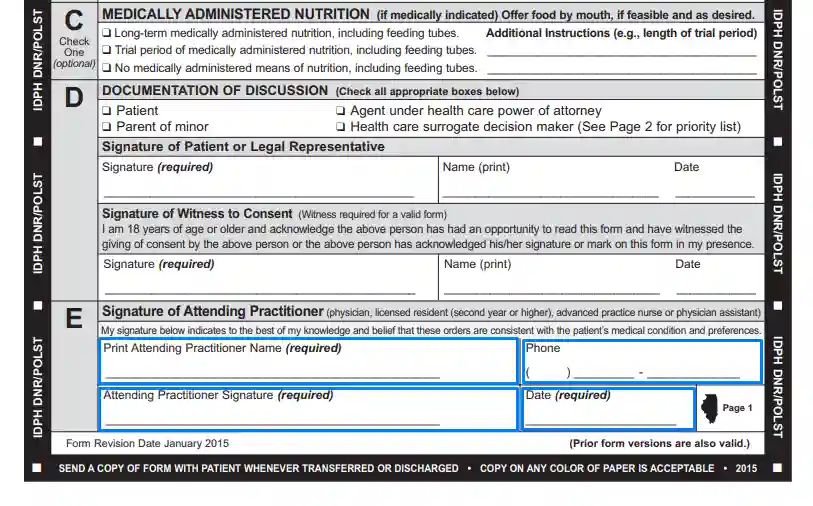
7. Approval of the Form’s Validity by a Practitioner
The physician treating the patient should fill out part E of the form. Specifically, the practitioner has to write the full name, emergency phone number, signature, and the date of the form’s execution.
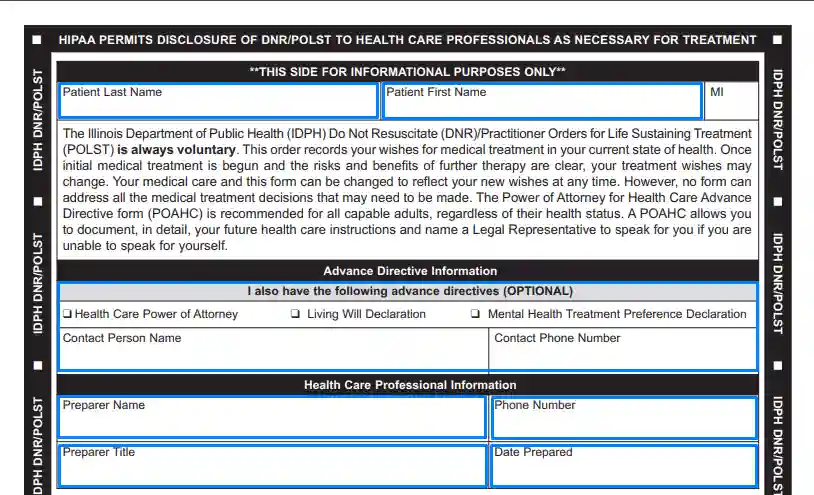
8. Fill Out the Informational Part of the Form
Complete the second side of the form by entering the patient’s first and second names, additional directives to the patient’s treatment, and personal data about the medical worker who was working with this form.
If you complete the DNR/POLST form correctly and the physician agrees to sign it, all healthcare workers treating the patient will comply with the conditions stated in the paper.