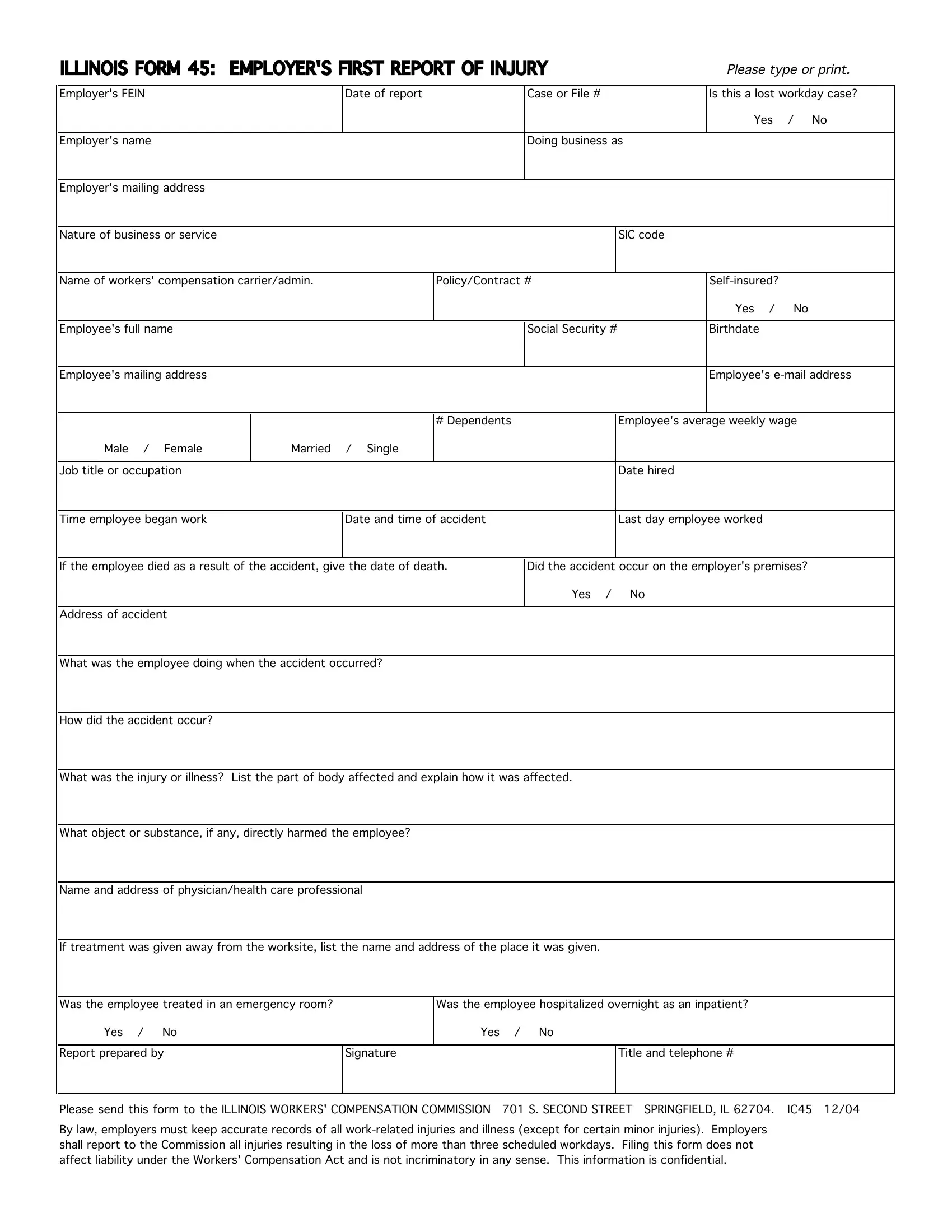
The Illinois 45 form, officially titled "Employer's First Report of Injury," serves as a crucial document within the sphere of workers' compensation in Illinois. Developed for the meticulous documentation of workplace injuries, this form requires employers to provide comprehensive details concerning an incident, including the employer's Federal Employer Identification Number (FEIN), the business name and address, the nature of the business, and specific information regarding the injured employee—ranging from their personal information to the specifics of their employment, injury particulars, and subsequent care. Additionally, it inquires whether the case resulted in lost workdays, thus signaling the severity of the incident. The legal mandate for this form underscores the importance of employer accountability in reporting injuries that lead to more than three days of work absenteeism, reinforcing the framework intended to protect worker rights and ensure timely and adequate compensation for work-related injuries. Importantly, completing and filing this form with the Illinois Workers' Compensation Commission does not presuppose liability under the Workers' Compensation Act, nor is it meant to be self-incriminating. Rather, it functions within a larger system designed to streamline the reporting process, maintain accurate records of work-related injuries, and facilitate a transparent communication channel between employers, employees, and the regulatory body overseeing workers' compensation claims. By emphasizing confidentiality, the form respects the privacy considerations of all involved parties, making it a fundamental facet of workplace safety and health administration in Illinois.
| Question | Answer |
|---|---|
| Form Name | Illinois Form 45 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | illinois form 45 pdf, form 45 illinois, ill form 45, illinois 45 form |
ILLINOIS FORM 45: EMPLOYER'S FIRST REPORT OF INJURY
Please type or print.
Employer's FEIN
Employer's name
Date of report |
Case or File # |
Is this a lost workday case? |
Yes / No
Doing business as
Employer's mailing address
Nature of business or service
SIC code
Name of workers' compensation carrier/admin. |
Policy/Contract # |
Yes / No
Employee's full name |
Social Security # |
Birthdate |
|
|
|
Employee's mailing address
Employee's
|
|
# Dependents |
Employee's average weekly wage |
Male / Female |
Married / Single |
|
|
|
|
|
|
Job title or occupation |
|
|
Date hired |
Time employee began work
Date and time of accident
Last day employee worked
If the employee died as a result of the accident, give the date of death. |
Did the accident occur on the employer's premises? |
Yes / No
Address of accident
What was the employee doing when the accident occurred?
How did the accident occur?
What was the injury or illness? List the part of body affected and explain how it was affected.
What object or substance, if any, directly harmed the employee?
Name and address of physician/health care professional
If treatment was given away from the worksite, list the name and address of the place it was given.
Was the employee treated in an emergency room? |
|
Was the employee hospitalized overnight as an inpatient? |
||
Yes / No |
|
Yes |
/ No |
|
|
|
|
|
|
Report prepared by |
Signature |
|
|
Title and telephone # |
|
|
|
|
|
Please send this form to the ILLINOIS WORKERS' COMPENSATION COMMISSION |
701 S. SECOND STREET SPRINGFIELD, IL 62704. IC45 12/04 |
|||
By law, employers must keep accurate records of all