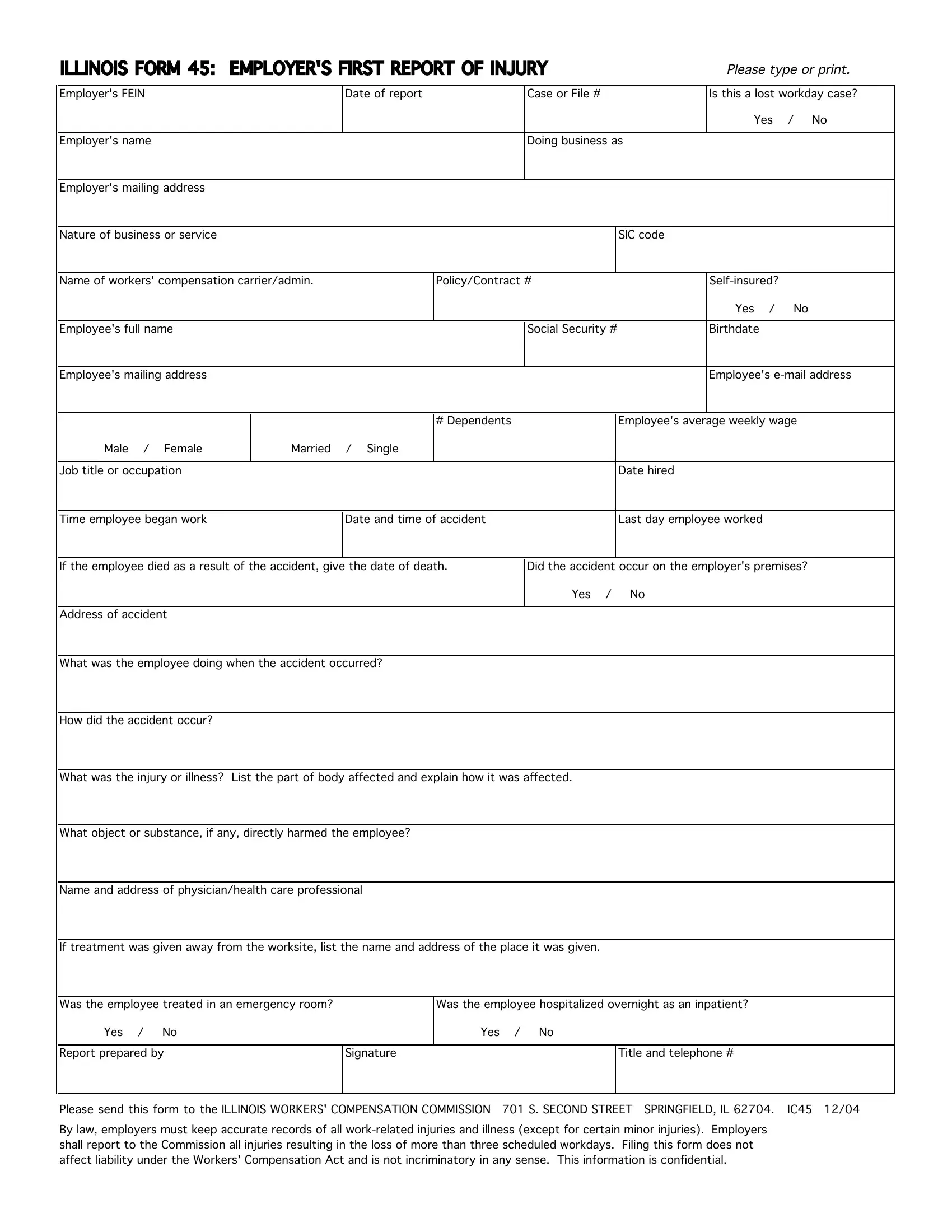
The Illinois 45 form, officially titled "Employer's First Report of Injury," serves as a crucial document within the sphere of workers' compensation in Illinois. Developed for the meticulous documentation of workplace injuries, this form requires employers to provide comprehensive details concerning an incident, including the employer's Federal Employer Identification Number (FEIN), the business name and address, the nature of the business, and specific information regarding the injured employee—ranging from their personal information to the specifics of their employment, injury particulars, and subsequent care. Additionally, it inquires whether the case resulted in lost workdays, thus signaling the severity of the incident. The legal mandate for this form underscores the importance of employer accountability in reporting injuries that lead to more than three days of work absenteeism, reinforcing the framework intended to protect worker rights and ensure timely and adequate compensation for work-related injuries. Importantly, completing and filing this form with the Illinois Workers' Compensation Commission does not presuppose liability under the Workers' Compensation Act, nor is it meant to be self-incriminating. Rather, it functions within a larger system designed to streamline the reporting process, maintain accurate records of work-related injuries, and facilitate a transparent communication channel between employers, employees, and the regulatory body overseeing workers' compensation claims. By emphasizing confidentiality, the form respects the privacy considerations of all involved parties, making it a fundamental facet of workplace safety and health administration in Illinois.
| Question | Answer |
|---|---|
| Form Name | Illinois Form 45 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | illinois form 45 pdf, form 45 illinois, ill form 45, illinois 45 form |