

Once you open the online editor for PDFs by FormsPal, you can easily fill out or change edit for for no download here and now. To maintain our tool on the forefront of convenience, we aim to put into practice user-oriented features and enhancements on a regular basis. We're always grateful for any suggestions - join us in revampimg the way you work with PDF forms. Getting underway is easy! All that you should do is stick to the following simple steps below:
Step 1: Just click on the "Get Form Button" above on this webpage to see our pdf form editor. This way, you'll find all that is necessary to fill out your file.
Step 2: After you access the tool, you will find the document ready to be completed. Apart from filling out various blanks, you may as well perform several other actions with the file, specifically writing any textual content, changing the initial textual content, adding graphics, affixing your signature to the form, and much more.
When it comes to fields of this particular document, here is what you need to know:
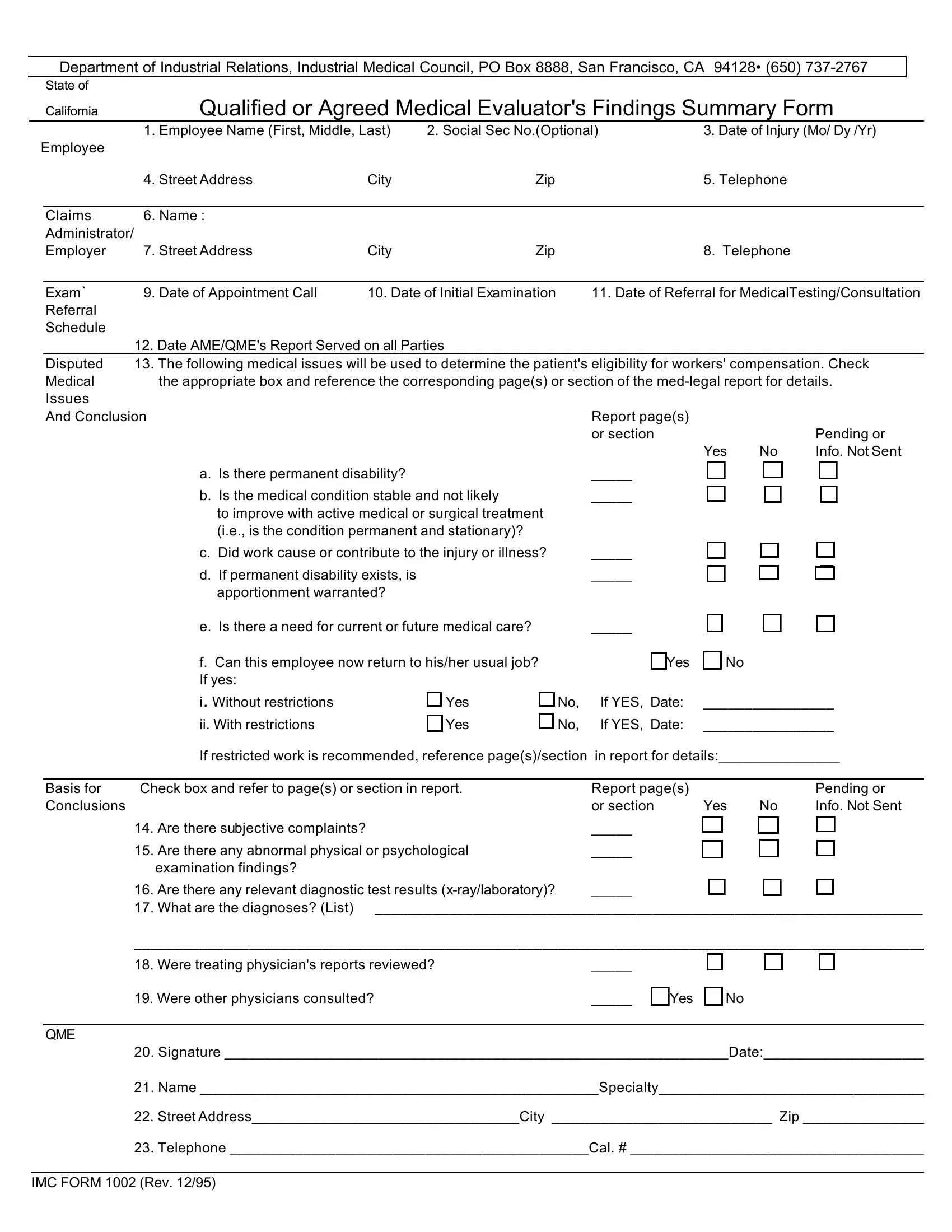
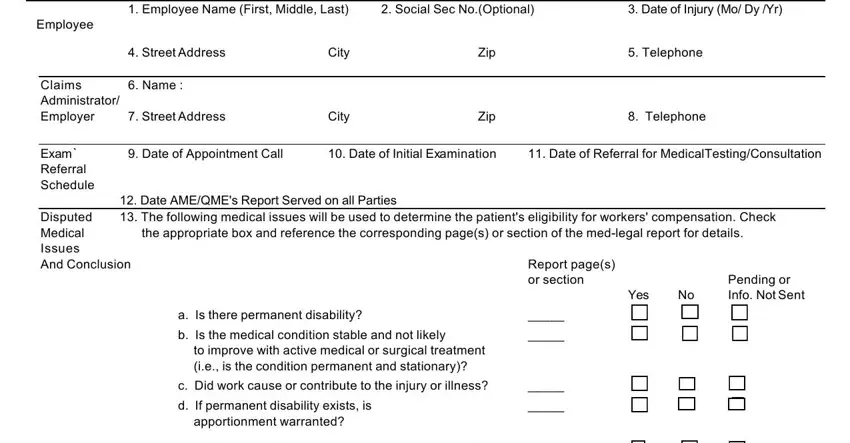
1. To start off, when filling in the edit for for no download, start in the form section that includes the subsequent blank fields:
2. Once your current task is complete, take the next step – fill out all of these fields - e Is there a need for current or, f Can this employee now return to, Basis for Check box and refer to, Yes, Yes, Are there subjective complaints, Yes, No If YES Date, No If YES Date, Report pages or section, Yes, Pending or Info Not Sent, If restricted work is recommended, Are there any relevant diagnostic, and Were treating physicians reports with their corresponding information. Make sure to double check that everything has been entered correctly before continuing!
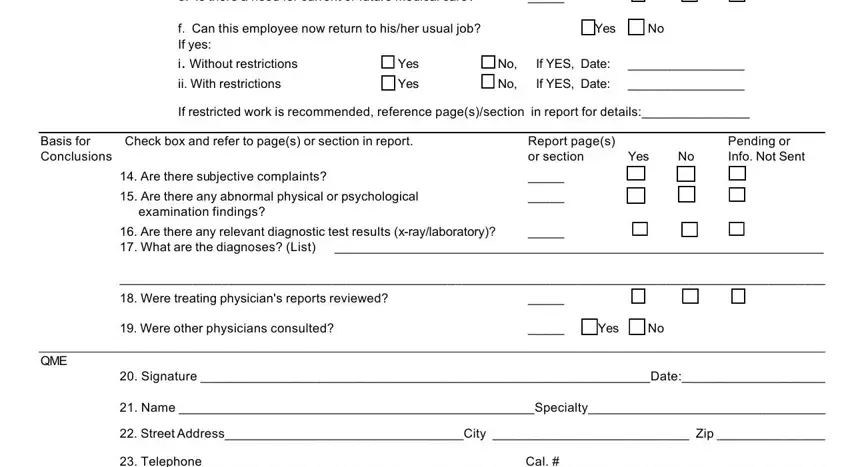
Concerning e Is there a need for current or and Are there subjective complaints, make certain you double-check them here. The two of these are certainly the key ones in this document.
Step 3: Before getting to the next stage, make certain that form fields are filled out correctly. When you believe it is all fine, press “Done." Create a 7-day free trial subscription with us and obtain instant access to edit for for no download - accessible from your personal account. Here at FormsPal.com, we endeavor to make sure that all your information is kept secure.