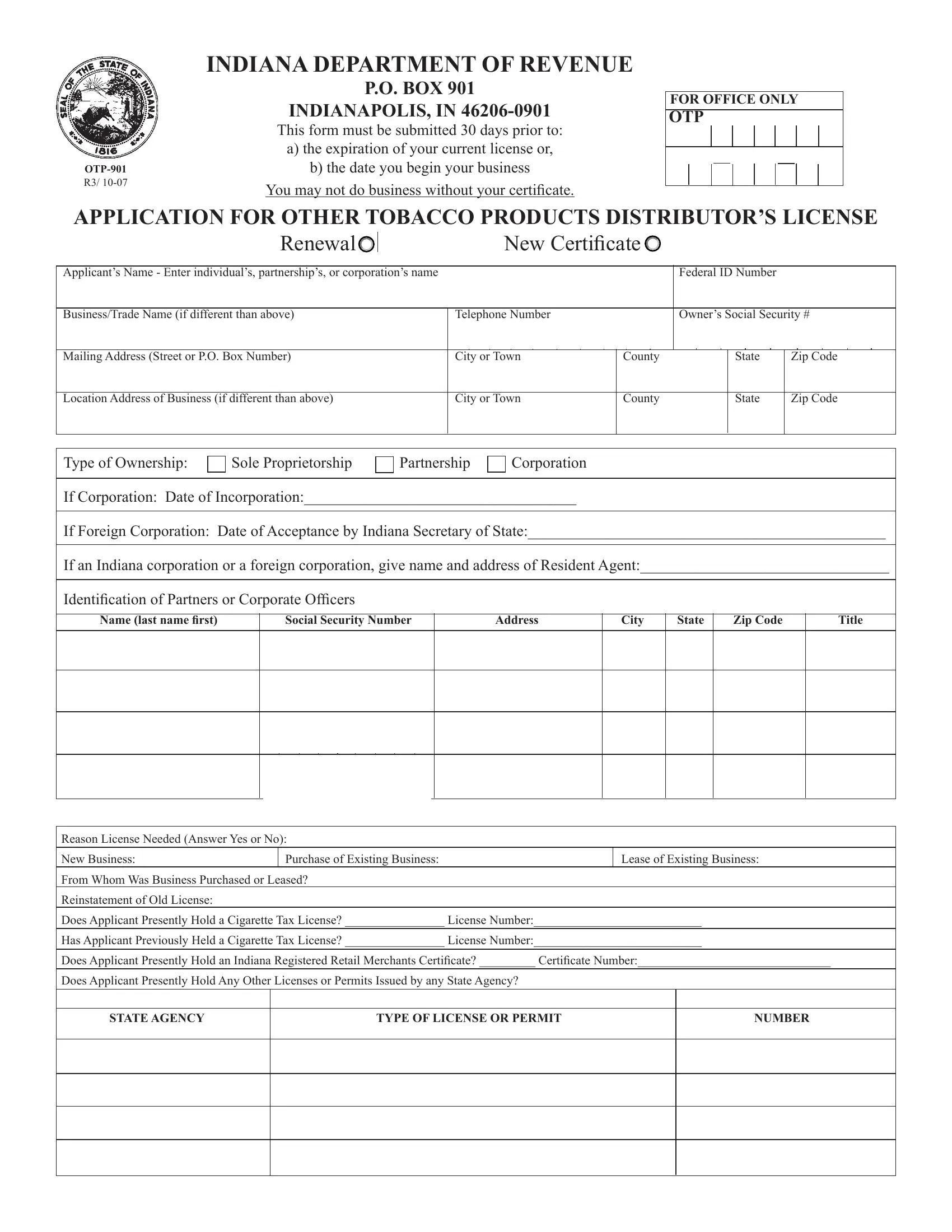
In the state of Indiana, businesses involved in the distribution of tobacco products are required to navigate through a comprehensive regulatory framework to ensure they operate within the confines of the law. One of the pivotal documents in this regulatory process is the Indiana Department of Revenue's OTP-901 form. This form, mandatory for entities engaged in the distribution of "other tobacco products", acts as an application for obtaining a distributor’s license. It must be submitted at least 30 days before the expiration of the current license or the commencement date of the business operations, underscoring the department's stringent timeline to maintain legal status. The form demands a detailed provision of information, spanning the applicant's identification details, type of ownership, and specifics about the business including its location, ownership structure, and the nature of the license sought – whether it’s a new application, a renewal, or a certificate for a new business. Crucially, it delves into the applicant's tax compliance status, asking about any previous or current cigarette tax licenses, and any other permits held that have been issued by state agencies. Additionally, the form also serves as a prerequisite for ensuring that the business has a sound record-keeping system for audit purposes and outlines the expectation for interstate sales, all while emphasizing adherence to the state's strict guidelines under the threat of perjury. This document exemplifies the meticulous steps a business must take to align with Indiana’s regulatory framework and highlights the importance of accuracy and timeliness in submissions.
| Question | Answer |
|---|---|
| Form Name | Indiana Otp 901 Form |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | otp901 indiana otp 901 renewal form |
INDIANA DEPARTMENT OF REVENUE
R3/
P.O. BOX 901
INDIANAPOLIS, IN
This form must be submitted 30 days prior to:
a)the expiration of your current license or,
b)the date you begin your business
You may not do business without your certificate.
FOR OFFICE ONLY
OTP
APPLICATION FOR OTHER TOBACCO PRODUCTS DISTRIBUTOR’S LICENSE
|
|
Renewal |
|
|
|
|
New Certificate |
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Applicant’s Name - Enter individual’s, partnership’s, or corporation’s name |
|
|
|
|
|
|
Federal ID Number |
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Business/Trade Name (if different than above) |
|
|
|
Telephone Number |
|
|
|
Owner’s Social Security # |
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Mailing Address (Street or P.O. Box Number) |
|
|
|
City or Town |
County |
|
|
State |
Zip Code |
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Location Address of Business (if different than above) |
|
|
|
City or Town |
County |
|
|
State |
Zip Code |
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Type of Ownership: |
|
Sole Proprietorship |
|
|
Partnership |
|
Corporation |
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
If Corporation: Date of Incorporation:___________________________________
If Foreign Corporation: Date of Acceptance by Indiana Secretary of State:______________________________________________
If an Indiana corporation or a foreign corporation, give name and address of Resident Agent:________________________________
Identifi cation of Partners or Corporate Officers
Name (last name fi rst)
Social Security Number
Address
City
State |
Zip Code |
|
|
Title
Reason License Needed (Answer Yes or No):
New Business: |
Purchase of Existing Business: |
Lease of Existing Business: |
From Whom Was Business Purchased or Leased?
Reinstatement of Old License:
Does Applicant Presently Hold a Cigarette Tax License? ________________ License Number:___________________________
Has Applicant Previously Held a Cigarette Tax License? ________________ License Number:___________________________
Does Applicant Presently Hold an Indiana Registered Retail Merchants Certifi cate? _________ Certificate Number:_______________________________
Does Applicant Presently Hold Any Other Licenses or Permits Issued by any State Agency?
STATE AGENCY
TYPE OF LICENSE OR PERMIT
NUMBER
Audit Information:
Location Where Records Will Be Available For Audit:
Phone Number of Location Of Audit Records:
Phone Number of Business Location:
Indicate Address of Each Location In Which You Have Other Tobacco Products in Storage
Location
OTP License Number
Indicate Name, Address, Phone Number and Estimated Annual Purchases from Whom You Currently Purchase and/or Expect to Purchase Other Tobacco Products: (A Computer Generated List Which Includes All Requested Information Will Be Accepted)
Supplier’s Name
Address
Phone Number
Estimated Annual Purchases
TOTAL:
If Necessary Attach Additional List.
Does Your Company Expect to Sell Other Tobacco Products Into Another State?___________________________________________________________________
List States: _________________________________________________________________________________________________________________________
Today’s Date
I declare under penalties of perjury that the information contained in this application and any attachments is true, correct and complete to the best of my knowledge and belief.
Signature of Taxpayer or Authorized Agent, Title |
Telephone Number |