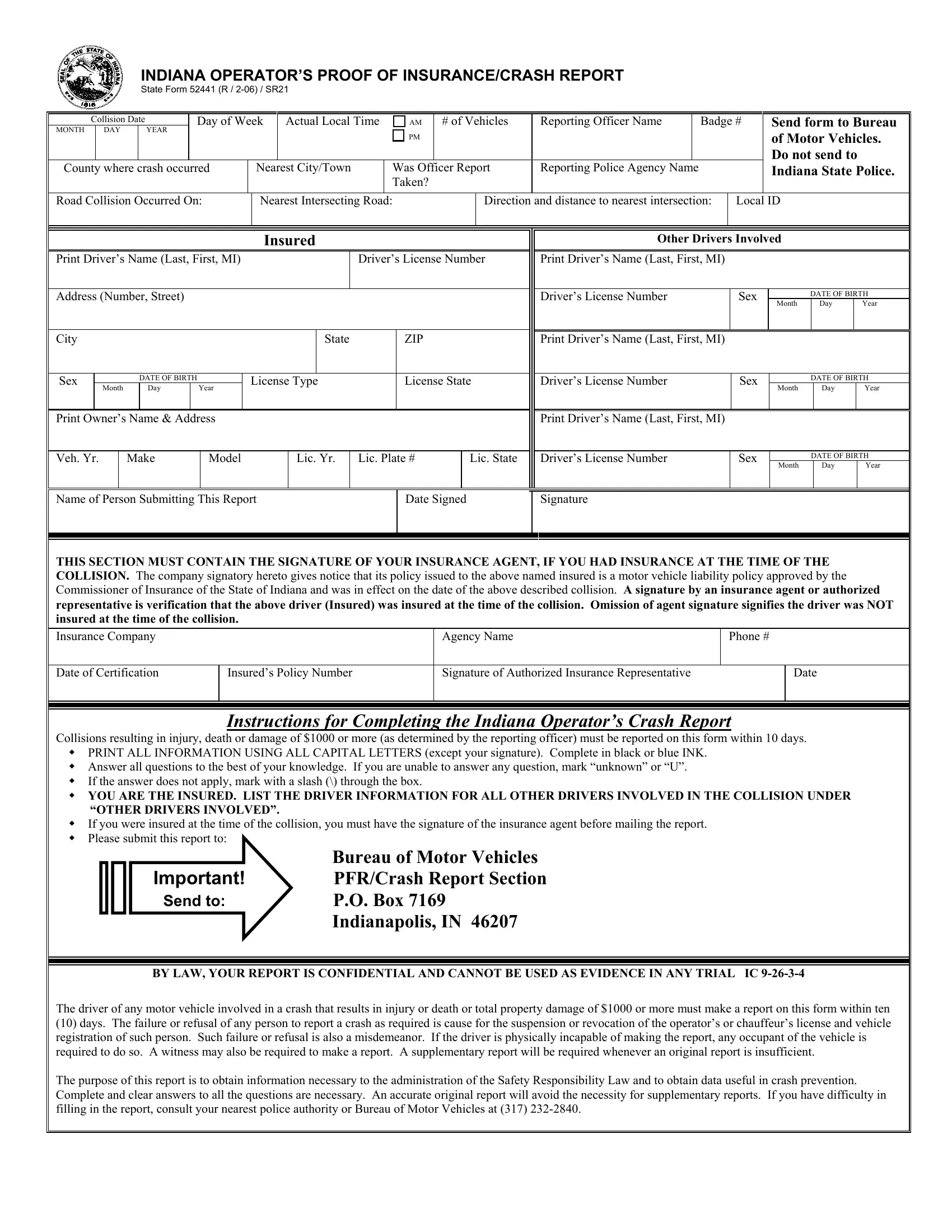

In a motor vehicle accident in Indiana that results in injury, death, or property damage totaling $1,000 or more, it is mandatory to complete and submit the Indiana Operator’s Proof of Insurance/Crash Report, commonly referred to as the SR21 form.
1. Write the Date and Time of the Collision
Start by writing the exact date (month, day, year) and the actual local time when the collision occurred. Specify whether it happened in the AM or PM.
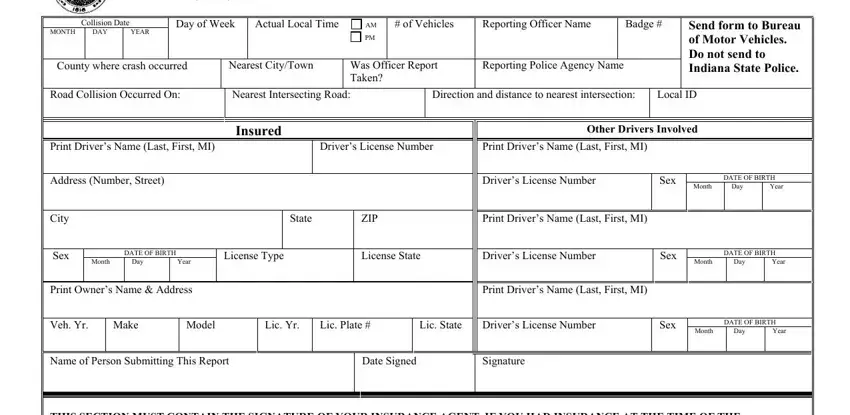
2. Add Location and Officer Details
Record the county where the crash occurred, the nearest city or town, and whether an officer's report was taken at the scene. Include the reporting officer’s name and badge number.
3. Describe the Collision Scene
Detail the road where the collision occurred, the nearest intersecting road, and the direction and distance to the nearest intersection. You will also need to enter the local ID if available.
4. List All Drivers Involved
For yourself and each driver involved in the accident, provide full names, dates of birth, driver’s license numbers, addresses, and vehicle information, including year, make, model, and license plate numbers.
5. Insurance Verification
This is a section where you must have your insurance agent sign to verify that you were insured at the time of the accident. Fill in the insurance company name, agency name, and phone number, along with the date of certification, policy number, and the signature of the authorized insurance representative.
6. Finalize the Report
Complete the report by printing the name of the person submitting it, signing it, and dating it. Ensure all information provided is printed in all capital letters using black or blue ink, except for the signatures.
7. Submit the Form
Send the completed form to the Bureau of Motor Vehicles, PFR/Crash Report Section at the address provided on the form. It is important to note that the form should not be sent to the Indiana State Police.