We have used the hard work of the best software engineers to build the PDF editor you are going to benefit from. Our software allows you to fill out the mydhr online portal interim change section file effortlessly and don’t waste valuable time. All you should do is comply with these particular straightforward recommendations.
Step 1: Select the button "Get Form Here".
Step 2: Now you can enhance the mydhr online portal interim change section. You need to use the multifunctional toolbar to add, eliminate, and change the content of the file.
These areas are in the PDF form you'll be filling out.
Write the details in Program Branch Worker ID Case, Case name, If you are not registered to vote, ZIP code, State, City, Phone number, Mailing address, City, State, ZIP code, Message number, Do you pay for housing c Yes, c No, and If yes complete below.
Type in the necessary information since you are within the Relationship to you, Sex circle one, Date of birth, Wants SNAP circle one, Purchase and prepare meals with, Self, M F, M F, M F, M F, M F, M F, M F, Y N, and Y N segment.
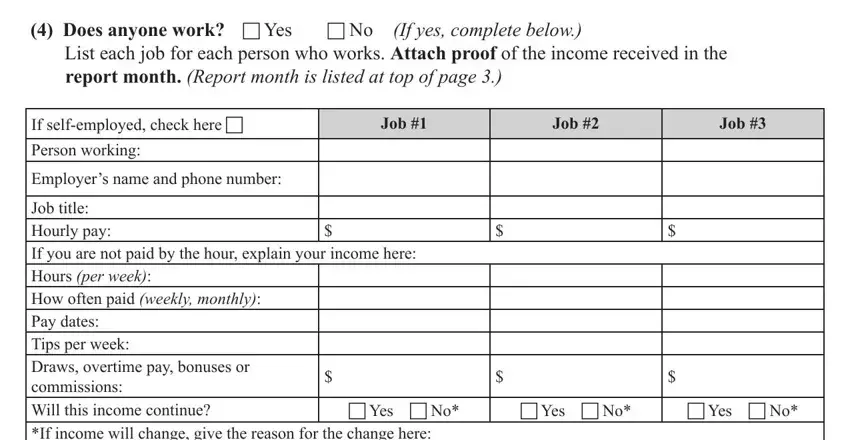
The Does anyone work c Yes List each, If yes complete below, c No, report month Report month is, If selfemployed check here c, Employers name and phone number, Job, Job, Job, Job title Hourly pay If you are, c Yes c No, If income will change give the, c Yes c No, and c Yes c No segment needs to be applied to note the rights or responsibilities of both sides.
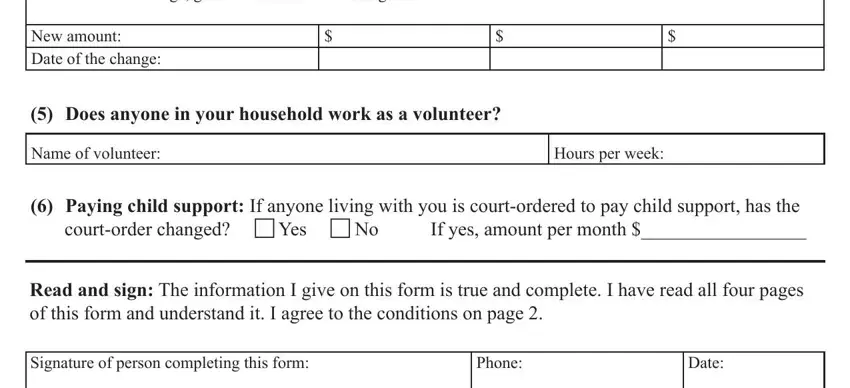
Finish by reading the next sections and preparing them accordingly: If income will change give the, New amount Date of the change, Does anyone in your household, Name of volunteer, Hours per week, Paying child support If anyone, Read and sign The information I, Signature of person completing, Phone, and Date.
Step 3: Select the "Done" button. Now you may upload your PDF form to your electronic device. Aside from that, it is possible to forward it by email.
Step 4: Make a copy of any document. It should save you time and enable you to stay away from problems in the future. Also, your data won't be shared or analyzed by us.
