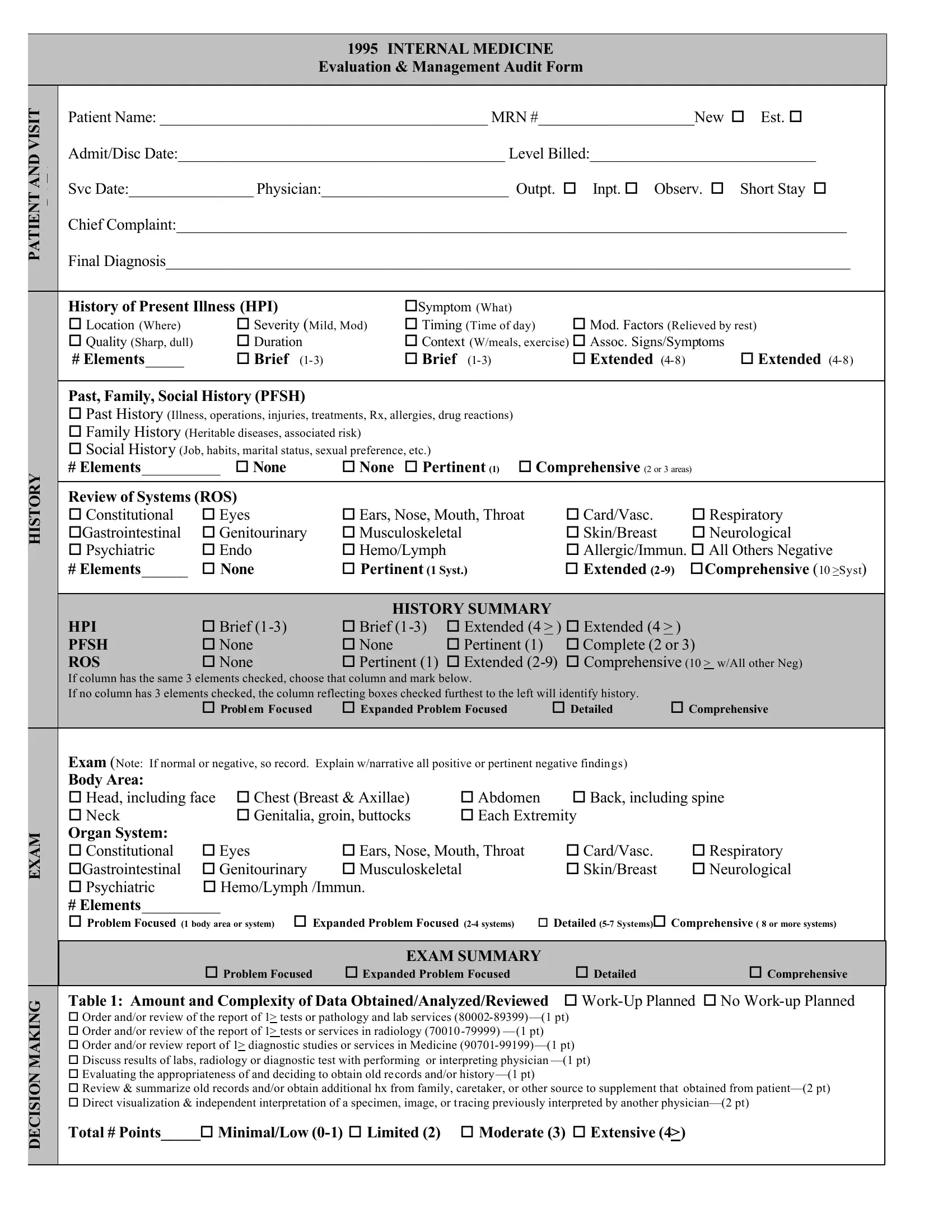
In the realm of healthcare, detailed and accurate documentation is a cornerstone not only for patient care but also for legal and billing purposes. The 1995 INTERNAL MEDICINE Evaluation & Management Audit Form plays a crucial role in this context, guiding physicians and healthcare providers through a comprehensive assessment of a patient's visit. Whether it's for a new or established patient, inpatient or outpatient care, this form encompasses several vital components including the patient's chief complaint, the history of present illness, with specifications such as symptoms, severity, duration, and factors that modify the condition. It also delves into the patient's past, family, and social history, review of systems across multiple bodily systems, and a detailed physical examination mapping from head to toe across organ systems. Not stopping at mere data collection, the form facilitates intricate medical decision-making through tables that evaluate the complexity of data, number of diagnoses or management options, and associated risks based on the patient's current condition. The summary of this audit form eventually aids in aligning the documented level of care with the actual services billed, ensuring that healthcare providers are accurately compensated for their services, while maintaining a clear and legal record of patient care.
| Question | Answer |
|---|---|
| Form Name | Internal Audit Medicine Form |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | internal audit printables form, audit printables printable, audit tools printables, audit printables fillable |
1995 INTERNAL MEDICINE
Evaluation & Management Audit Form
|
VISIT |
Patient Name: __________________________________________ MRN #____________________New o Est. o |
||||||||
|
|
|||||||||
|
AND |
Admit/Disc Date:__________________________________________ Level Billed:_____________________________ |
||||||||
|
Svc Date:________________ Physician:________________________ Outpt. o Inpt. o |
Observ. o Short Stay o |
||||||||
|
PATIENT |
|||||||||
|
Chief Complaint:______________________________________________________________________________________ |
|||||||||
|
|
|||||||||
|
|
Final Diagnosis________________________________________________________________________________________ |
||||||||
|
|
|
|
|
|
|
|
|
||
|
|
History of Present Illness (HPI) |
|
oSymptom (What) |
|
|
|
|
||
|
|
o Location (Where) |
o Severity (Mild, Mod) |
o Timing (Time of day) |
o Mod. Factors (Relieved by rest) |
|||||
|
|
o Quality (Sharp, dull) |
o Duration |
|
o Context (W/meals, exercise) o Assoc. Signs/Symptoms |
|||||
|
|
# Elements_____ |
o Brief |
|
o Brief |
|
o Extended |
o Extended |
||
|
|
|
|
|
|
|
|
|
|
|
|
|
Past, Family, Social History (PFSH) |
|
|
|
|
|
|
|
|
|
|
o Past History (Illness, operations, injuries, treatments, Rx, allergies, drug reactions) |
|
|
|
|
||||
|
|
o Family History (Heritable diseases, associated risk) |
|
|
|
|
|
|
||
|
|
o Social History (Job, habits, marital status, sexual preference, etc.) |
|
|
|
|
|
|||
|
HISTORY |
# Elements__________ o None |
o None |
o Pertinent (1) |
o Comprehensive (2 or 3 areas) |
|||||
|
|
|
|
|
|
|
|
|
|
|
|
Review of Systems (ROS) |
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
||
|
|
o Constitutional |
o Eyes |
o Ears, Nose, Mouth, Throat |
o Card/Vasc. |
|
o Respiratory |
|||
|
|
oGastrointestinal |
o Genitourinary |
o Musculoskeletal |
|
o Skin/Breast |
o Neurological |
|||
|
|
o Psychiatric |
o Endo |
o Hemo/Lymph |
|
|
o Allergic/Immun. o All Others Negative |
|||
|
|
# Elements______ |
o None |
o Pertinent (1 Syst.) |
|
o Extended |
oComprehensive (10 >Syst) |
|||
|
|
|
|
|
|
|
|
|||
|
|
|
|
HISTORY SUMMARY |
|
|
|
|||
|
|
HPI |
o Brief |
o Brief |
|
|||||
|
|
PFSH |
o None |
o None |
o Pertinent (1) |
o Complete (2 or 3) |
||||
|
|
ROS |
o None |
o Pertinent (1) o Extended |
o Comprehensive (10 > w/All other Neg) |
|||||
|
|
If column has the same 3 elements checked, choose that column and mark below. |
|
|
|
|
||||
|
|
If no column has 3 elements checked, the column reflecting boxes checked furthest to the left will identify history. |
|
|
||||||
|
|
|
o Problem Focused |
o Expanded Problem Focused |
o Detailed |
o Comprehensive |
||||
|
|
|
|
|
||||||
|
|
Exam (Note: If normal or negative, so record. Explain w/narrative all positive or pertinent negative findings) |
|
|
||||||
|
|
Body Area: |
|
|
|
|
|
|
|
|
|
|
o Head, including face o Chest (Breast & Axillae) |
o Abdomen |
o Back, including spine |
||||||
|
|
o Neck |
o Genitalia, groin, buttocks |
o Each Extremity |
|
|
||||
|
EXAM |
Organ System: |
|
|
|
|
|
|
|
|
|
o Constitutional |
o Eyes |
o Ears, Nose, Mouth, Throat |
o Card/Vasc. |
|
o Respiratory |
||||
|
|
|
||||||||
|
|
oGastrointestinal |
o Genitourinary |
o Musculoskeletal |
|
o Skin/Breast |
o Neurological |
|||
|
|
o Psychiatric |
o Hemo/Lymph /Immun. |
|
|
|
|
|
|
|
#Elements__________
|
|
o Problem Focused (1 body area or system) o Expanded Problem Focused |
o Detailed |
|||
|
|
|
|
|
|
|
|
|
|
EXAM SUMMARY |
|
|
|
|
|
o Problem Focused |
o Expanded Problem Focused |
|
o Detailed |
o Comprehensive |
|
MAKING |
Table 1: Amount and Complexity of Data Obtained/Analyzed/Reviewed |
o |
|||
|
o Order and/or review of the report of 1> tests or pathology and lab services |
|
||||
|
|
|
||||
|
|
o Order and/or review of the report of 1> tests or services in radiology |
|
|
||
|
|
o Order and/or review report of 1> diagnostic studies or services in Medicine |
|
|||
|
|
o Discuss results of labs, radiology or diagnostic test with performing or interpreting physician |
|
|||
|
DECISION |
o Evaluating the appropriateness of and deciding to obtain old records and/or |
|
|
|
|
|
o Review & summarize old records and/or obtain additional hx from family, caretaker, or other source to supplement that obtained from |
|||||
|
|
|||||
|
|
o Direct visualization & independent interpretation of a specimen, image, or tracing previously interpreted by another |
||||
|
|
Total # Points_____o Minimal/Low |
|
|||
|
|
|
|
|
|
|
|
|
Table 2: Number of DX or Management Options |
|
|
Number (B) X |
Points (C) = Results ( D) (Formula B X C =D) |
|
|
|
||||||||||||||||||||||||||||||||||
|
|
o |
|
|
(Max 2) |
|
|
|
1 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
|
|
o Established problem to examiner; stable, improved |
|
|
|
|
|
|
|
|
|
1 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
o Established problem to examiner; worsening |
|
|
|
|
|
|
|
|
|
|
|
|
2 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
o New problem to examiner; no additional workup |
|
|
|
|
|
(Max 1) |
|
|
|
3 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
o New problem to examiner; additional workup planned |
|
|
|
|
|
|
|
|
|
4 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Total |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
Total # Points______ |
|
|
|
|
o Minimal (<1) |
|
|
|
|
|
o Limited (2) |
|
o Multiple (3) |
o Extensive (>4) |
|
|
|
||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||
|
|
Table 3: Associated Risks: Overall measure of risk is highest level circled |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||
|
|
Level |
|
Presenting |
|
|
|
|
|
|
Diagnostic |
|
|
|
|
|
|
|
|
|
|
Medical |
|
|
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||
|
|
|
|
Problem |
|
|
|
|
|
|
|
|
|
Procedure |
|
|
|
|
|
|
|
|
|
|
Management |
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||
|
|
Minimal |
|
o One |
|
|
o Lab Tests requiring venipuncture |
|
|
|
|
|
|
o Rest, Gargles, Elastic Bandage |
|||||||||||||||||||||||||||||
|
|
|
|
e.g. cold, insect bite, tinea corporis |
|
|
Chest |
|
|
|
|
|
|
Superficial dressings |
|
|
|
|
|
||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Ultrasound, eg., echocardiography |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
KOH prep |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||
MAKING |
|
Low |
|
o 2 > |
|
|
o Physiologic tests not under stress |
|
|
|
|
|
|
o |
|
|
|
||||||||||||||||||||||||||
|
|
|
1 stable chronic illness |
|
|
|
|
|
|
|
|
|
Minor surgery w/no identified risks |
||||||||||||||||||||||||||||||
|
|
|
Acute uncomplicated illness or injury |
|
|
Superficial needle biopsies, clinical lab tests - |
|
|
|
|
Physical or Occupational Therapy |
||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Requiring arterial puncture, skin biopsies |
|
|
|
|
IV fluids w/o additives |
|
|
|
|||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||
|
Moderate |
|
o 1 > more chronic illness w/mild |
|
|
o Physiologic test under stress |
|
|
|
|
|
|
o Minor surgery w/ identified risks |
||||||||||||||||||||||||||||||
DECISION |
|
|
|
Exacerbation, progression, or side effects |
|
Dx endoscopies w/no identified risks |
|
|
|
|
|
|
Elective major surgery w/no |
|
|
|
|||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||
|
|
|
|
2 > more stable chronic illnesses |
|
|
Deep needle or incisional biopsy |
|
|
|
|
|
|
identified risks, prescription drug |
|||||||||||||||||||||||||||||
|
|
|
|
Undiagnosed new problem w/uncertain |
|
|
Cardiovascular imaging studies w/contrast |
|
|
|
|
management, therapeutic nuclear |
|||||||||||||||||||||||||||||||
|
|
|
|
Prognosis, acute illness w/systemic |
|
|
and no identified risk factors, obtain |
|
|
|
|
|
|
medicine, IV fluids w/additives |
|||||||||||||||||||||||||||||
|
|
|
|
Symptoms, Acute complicated injury |
|
|
fluid from body cavity |
|
|
|
|
|
|
|
|
|
Closed Tx fracture/dislocation |
|
|
|
|||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
W/o manipulation |
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||
|
|
High |
|
o 1 > more chronic illnesses with severe |
|
o Cardiovascular imaging studies w/contrast |
|
|
|
o Elective major surgery w/ident |
|||||||||||||||||||||||||||||||||
|
|
|
|
Exacerbation, progression, or side effects |
|
w/identified risk factors, Cardiac electro- |
|
|
|
|
factor, emergency major surgery |
||||||||||||||||||||||||||||||||
|
|
|
|
Of treatment, acute or chronic illnesses or |
|
physiological tests, diagnostic endoscopies |
|
|
|
|
parenteral controlled substances |
||||||||||||||||||||||||||||||||
|
|
|
|
Injuries that pose a threat to life or bodily |
|
w/identified risk factors discography |
|
|
|
|
|
|
drug tx requiring intensive monitor |
||||||||||||||||||||||||||||||
|
|
|
|
Function, an abrupt change neurologic |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
for toxicity, decision not to res- |
|||||||||||||||||||
|
|
|
|
Status. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
uscitate or |
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Poor prognosis |
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
|
Summary |
|
|
|
|
o Minimal |
|
|
|
|
|
|
|
|
o Low |
|
|
o Moderate |
o High |
|
|
|
|
|
|
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
SUMMARY OF MEDICAL DECISION MAKING TABLES |
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||
|
|
Complexity of Data |
? Minimal (<1) |
|
? Limited (2 ) |
|
? Moderate (3) |
|
|
|
? Extensive (>4) |
|
|
|
|||||||||||||||||||||||||||||
|
|
Management options |
? Minimal (<1) |
|
? Limited (2) |
|
? Multiple (3) |
|
|
|
|
? Extensive (>4) |
|
|
|
||||||||||||||||||||||||||||
|
|
Associated Risks |
|
|
|
? Minimal |
|
|
|
|
? Low |
|
|
|
|
? Moderate |
|
|
|
|
? High |
|
|
|
|
|
|
|
|
||||||||||||||
|
|
|
(Draw a line down column w/ |
|
|
|
|||||||||||||||||||||||||||||||||||||
|
|
TOTAL |
|
|
|
? Straight Forward |
|
? Low |
|
|
|
|
? Moderate |
|
|
|
|
? High |
|
|
|
|
|
|
|
|
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
E&M DOCUMENTATION SUMMARY |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
|
|
History |
? |
Problem Focused |
? |
Expanded Problem Focused |
? |
Detailed |
|
|
? |
Comprehensive |
? |
Comprehensive |
|||||||||||||||||||||||||||||
|
|
Exam |
? |
Problem Focused |
? |
Expanded Problem Focused |
? |
Detailed |
|
|
? |
Comprehensive |
? |
Comprehensive |
|||||||||||||||||||||||||||||
|
|
Decision Making |
? |
Straight Forward |
? |
Straight Forward |
|
|
|
? |
Low Complex |
? |
Moderate |
? |
High Complexity |
||||||||||||||||||||||||||||
SUMMARY |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
Initial |
|
|
|
IP Sub Care |
|
|
New Outpatient and |
|
|
|
|
|
Outpatient Established |
|
|
|
||||||||||||||||||||||
|
|
|
|
|
Inpt./Observ |
|
|
|
FU Consults |
|
|
IP/OP Consults |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
History |
|
|
|
D |
|
C |
|
C |
|
|
PF |
EFP |
|
|
D |
|
PF |
|
EPF |
|
D |
|
C |
|
C |
|
|
|
|
PF |
|
EPF |
|
D |
|
C |
|
|
|||
|
|
(Interval Hx - Sub) |
|
|
or |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
AUDIT |
|
|
|
|
|
C |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
C |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
Examination |
|
|
|
D |
|
C |
|
C |
|
|
PF |
EFP |
|
|
D |
|
PF |
|
EPF |
|
D |
|
C |
|
C |
|
|
|
|
PF |
|
EPF |
|
D |
|
C |
|
|
|||
|
|
|
|
|
|
|
or |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Medical Decision |
|
|
|
SF/ |
|
M |
|
H |
|
|
SF/ |
M |
|
|
|
|
H |
|
SF |
|
SF |
|
L |
|
M |
|
H |
|
|
|
|
SF |
|
L |
|
M |
|
H |
|
|
|
|
|
|
|
|
|
|
L |
|
|
|
|
|
|
L |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Level |
|
|
1 |
|
2 |
|
3 |
|
1 |
2 |
|
|
|
|
3 |
1 |
|
2 |
|
3 |
|
4 |
|
5 |
|
1 |
|
2 |
|
3 |
|
4 |
|
5 |
|
|
|||||
|
|
Comments: |
Level Billed_____________ |
|
|
Level Documented_____________ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|