The Iowa Cremation Authorization form is a pivotal document for those looking to arrange a cremation within Cedar Rapids, Iowa, explicitly detailing the process and legalities involved. It serves as a formal request and permission for Iowa Cremation, or its acting agent, to cremate the remains of the designated individual, subject to the establishment's rules and regulations. The authorization form ensures clarity in the responsibilities and rights of the authorizing agent(s), including the indemnity clause which protects the crematory against claims arising from the cremation process, inaccuracies in identification, and handling of the decedent's remains. It outlines specific instructions for handling valuables, determining the final disposition of the remains, and acknowledges the authorizing person's comprehension and acceptance of the cremation process. The form also emphasizes the legal standing of the authorizing person(s), confirming their authority under Iowa law to make such decisions. Additionally, it addresses the conditions under which cremation can proceed or be halted, the responsibilities regarding the disposition of the cremated remains if not claimed, and the technical aspects of the cremation process, including the handling of medical devices that could pose hazards. The thorough documentation and requirement for multiple signatures underscore the seriousness and irreversible nature of the cremation decision, ensuring that all parties are well-informed and in agreement.
| Question | Answer |
|---|---|
| Form Name | Iowa Cremation Authorization Form |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | cremation authorization iowa cremation authorization forms |
Iowa Cremation
4200 1st Ave NE Cedar Rapids, IA 52402
License#: 00601
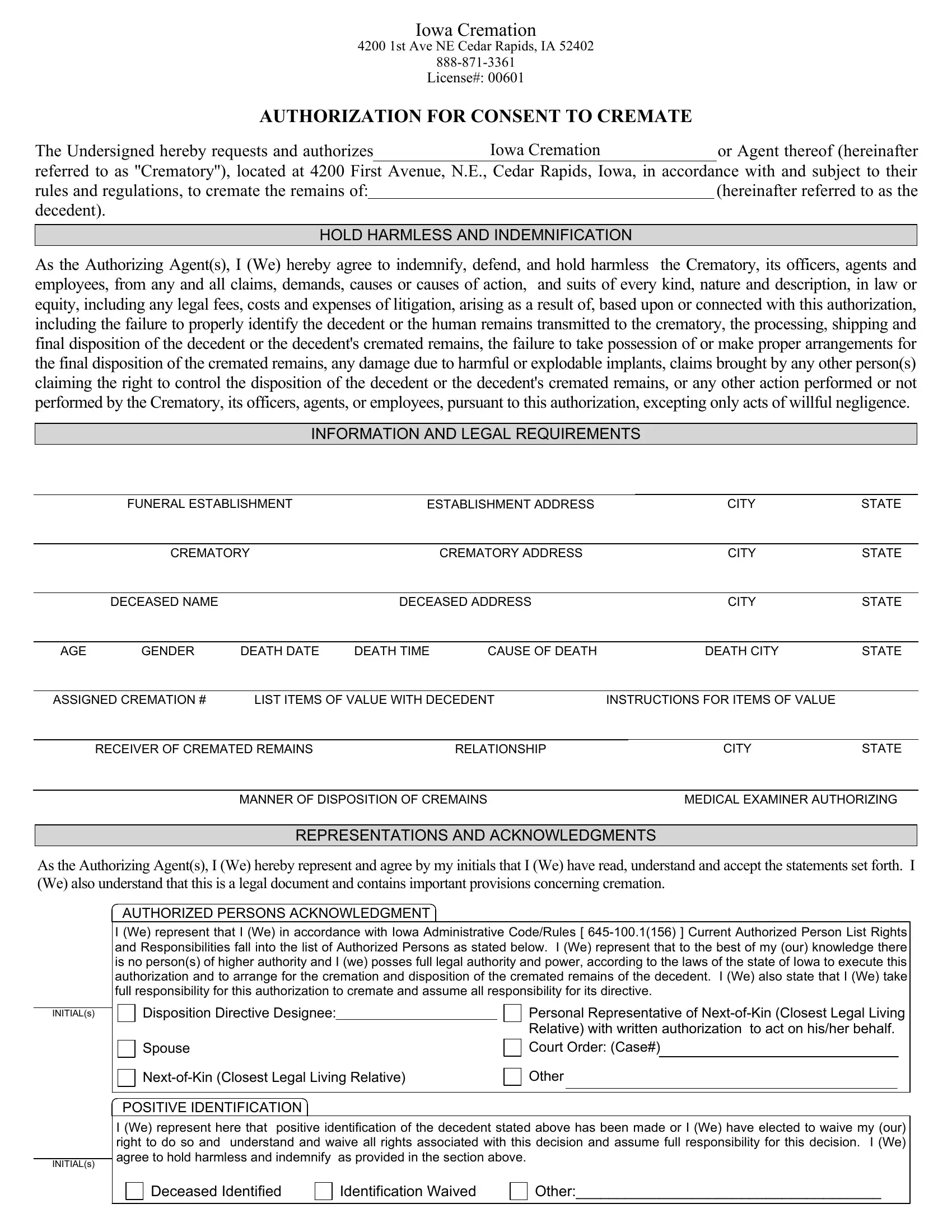
AUTHORIZATION FOR CONSENT TO CREMATE
The Undersigned hereby requests and authorizes Iowa Cremation or Agent thereof (hereinafter
referred to as ''Crematory''), located at 4200 First Avenue, N.E., Cedar Rapids, Iowa, in accordance with and subject to their
rules and regulations, to cremate the remains of: |
(hereinafter referred to as the |
|
decedent). |
|
|
|
|
|
HOLD HARMLESS AND INDEMNIFICATION |
|
|
As the Authorizing Agent(s), I (We) hereby agree to indemnify, defend, and hold harmless the Crematory, its officers, agents and employees, from any and all claims, demands, causes or causes of action, and suits of every kind, nature and description, in law or equity, including any legal fees, costs and expenses of litigation, arising as a result of, based upon or connected with this authorization, including the failure to properly identify the decedent or the human remains transmitted to the crematory, the processing, shipping and final disposition of the decedent or the decedent's cremated remains, the failure to take possession of or make proper arrangements for the final disposition of the cremated remains, any damage due to harmful or explodable implants, claims brought by any other person(s) claiming the right to control the disposition of the decedent or the decedent's cremated remains, or any other action performed or not performed by the Crematory, its officers, agents, or employees, pursuant to this authorization, excepting only acts of willful negligence.
INFORMATION AND LEGAL REQUIREMENTS
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
FUNERAL ESTABLISHMENT |
|
|
ESTABLISHMENT ADDRESS |
|
|
CITY |
STATE |
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
CREMATORY |
|
|
|
CREMATORY ADDRESS |
|
|
CITY |
STATE |
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DECEASED NAME |
|
|
|
|
DECEASED ADDRESS |
|
|
CITY |
STATE |
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
AGE |
|
GENDER |
DEATH DATE |
DEATH TIME |
CAUSE OF DEATH |
|
|
DEATH CITY |
STATE |
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
||||||
|
ASSIGNED CREMATION # |
LIST ITEMS OF VALUE WITH DECEDENT |
|
INSTRUCTIONS FOR ITEMS OF VALUE |
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
RECEIVER OF CREMATED REMAINS |
|
|
|
RELATIONSHIP |
|
|
CITY |
STATE |
||||
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
MANNER OF DISPOSITION OF CREMAINS |
|
|
MEDICAL EXAMINER AUTHORIZING |
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
REPRESENTATIONS AND ACKNOWLEDGMENTS
As the Authorizing Agent(s), I (We) hereby represent and agree by my initials that I (We) have read, understand and accept the statements set forth. I (We) also understand that this is a legal document and contains important provisions concerning cremation.
INITIAL(s)
INITIAL(s)
AUTHORIZED PERSONS ACKNOWLEDGMENT
I (We) represent that I (We) in accordance with Iowa Administrative Code/Rules [
|
Disposition Directive Designee: |
|
Personal Representative of |
||||||
|
|
|
|
|
|
Relative) with written authorization to act on his/her behalf. |
|||
|
|
|
|
|
|
||||
|
|
|
|
|
|
Court Order: (Case#) |
|||
|
Spouse |
|
|||||||
|
|
Other |
|
|
|||||
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
POSITIVE IDENTIFICATION
I (We) represent here that positive identification of the decedent stated above has been made or I (We) have elected to waive my (our) right to do so and understand and waive all rights associated with this decision and assume full responsibility for this decision. I (We) agree to hold harmless and indemnify as provided in the section above.
Deceased Identified |
|
Identification Waived |
|
Other:_____________________________________ |
CREMATION AUTHORIZATION
Page 2 of 2
REPRESENTATIONS AND ACKNOWLEDGMENTS
As the Authorizing Agent(s), I (We) hereby represent and agree by my (our) initials that I (we) have read, understand and accept the statements set forth. I (we) also understand that this is a legal document and contains important provisions concerning cremation.
INITIAL(s)
CREMATION ACKNOWLEDGEMENT
I (We) represent here that I (We) understand I (We) have the right to revoke this authorization and instruct the crematory to cancel the cremation provided such instruction is received in writing prior to the beginning of the cremation. In the event the cremation has been started, the authorization stands and we hold harmless all parties involved directly or indirectly with the the Crematory resulting from this cremation. I (We) also acknowledge and understand that in the event there is written notification prior to the start of the cremation that a person(s) of suspected equal or superior right exists and/or opposes the cremation, the Crematory reserves the right to delay the cremation until such time the matter is resolved in a manner acceptable to the Crematory or a court order is presented authorizing the cremation. In such an event, or in order to comply with the laws of this state, the Crematory reserves the right to preserve the remains in accordance with current laws in this state which may include refrigeration and/or arterial or hypodermic embalming. If embalming is performed to comply with current State Laws I (We) do hereby grant permission and understand I (we) may be liable for additional charges that pertain as listed on the current General Price List.
INITIAL(s)
DISPOSITION RESPONSIBILITY
I (We) understand that in accordance with Iowa Administrative Code/Rules [
INITIAL(s)
CREMATION PROCESS ACKNOWLEDGMENT
I (We) represent and understand that cremation is performed by placing the decedent in a cremation container or on a cremation tray and then placing the cremation container or tray into a cremation chamber or retort where they are subjected to intense heat and flame. Through the use of natural gas, incineration of the container and its contents is accomplished and all substances are consumed, except bone fragments (calcium compounds) and metal (including gold and silver and other
INITIAL(s)
MEDICAL DEVICES
I (We) represent here that to the best of my/our knowledge there are no medical devices, materials, or implants that may be explosive or potentially hazardous to equipment or persons performing the cremation. In the event the decedent does have such a device, I (We) authorize the removal of such devices as deemed necessary by the crematory to prevent harm to equipment or person and understand these items will be discarded as deemed appropriate by the crematory and will not be returned.
I (WE) ACKNOWLEDGE THAT BY EXECUTING THIS CREMATION AUTHORIZATION THAT I (WE) HAVE READ AND FULLY UNDERSTAND PAGES 1 AND 2 OF SAID AUTHORIZATION AND ACKNOWLEDGE AND UNDERSTAND THE HOLD HARMLESS AND INDEMNIFICATION PROVISION. FURTHER, ALL REPRESENTATIONS AND STATEMENTS CONTAINED WITHIN THIS AUTHORIZATION ARE TRUE AND CORRECT.
|
|
|
|
PRINT NAME |
RELATIONSHIP |
SIGNATURE |
DATE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PRINT NAME |
RELATIONSHIP |
SIGNATURE |
DATE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PRINT NAME |
RELATIONSHIP |
SIGNATURE |
DATE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PRINT NAME |
RELATIONSHIP |
SIGNATURE |
DATE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PRINT NAME |
RELATIONSHIP |
SIGNATURE |
DATE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
FUNERAL DIRECTOR NAME |
LICENSE NUMBER |
SIGNATURE |
DATE |