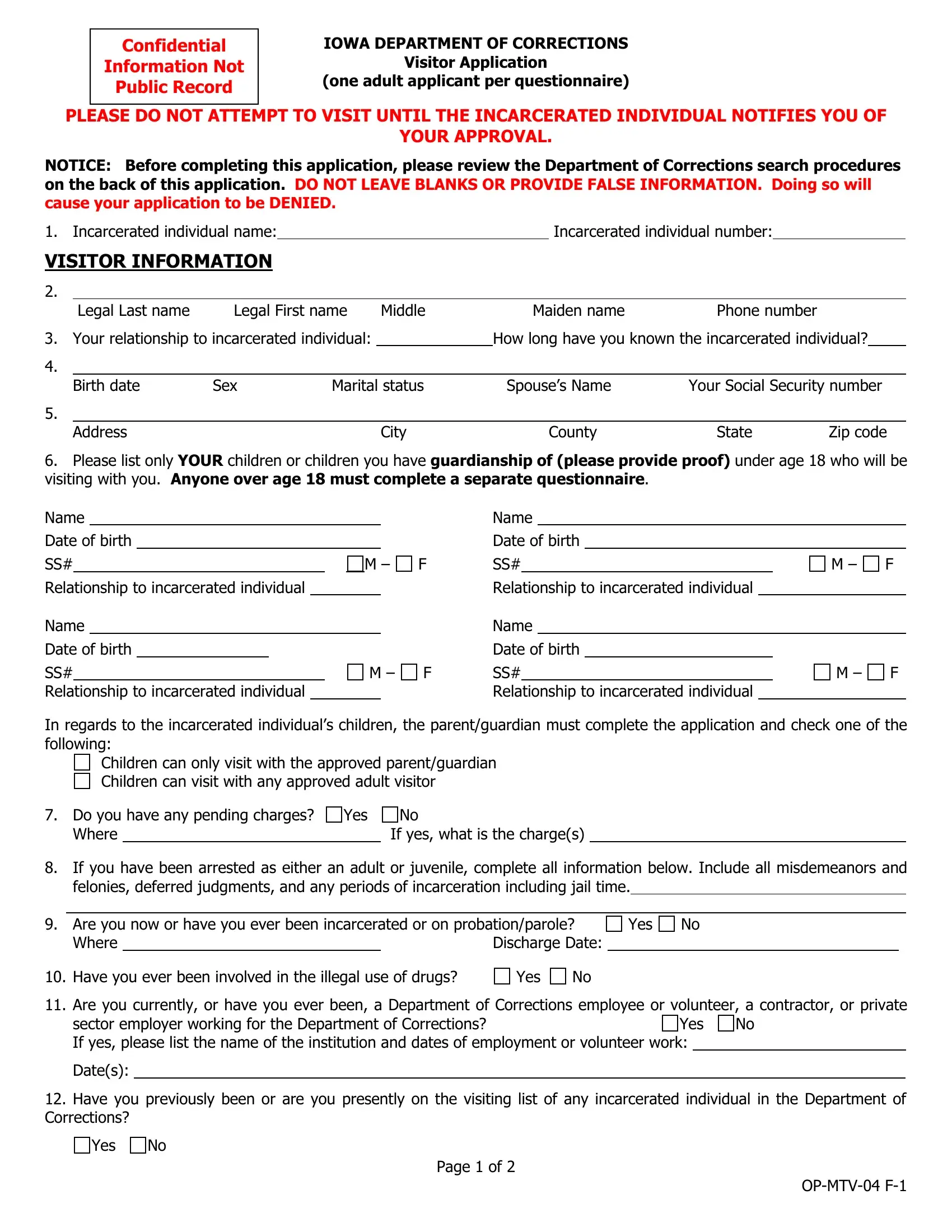
Confidential |
IOWA DEPARTMENT OF CORRECTIONS |
Information Not |
Visitor Application |
Public Record |
(one adult applicant per questionnaire) |
PLEASE DO NOT ATTEMPT TO VISIT UNTIL THE INCARCERATED INDIVIDUAL NOTIFIES YOU OF
YOUR APPROVAL.
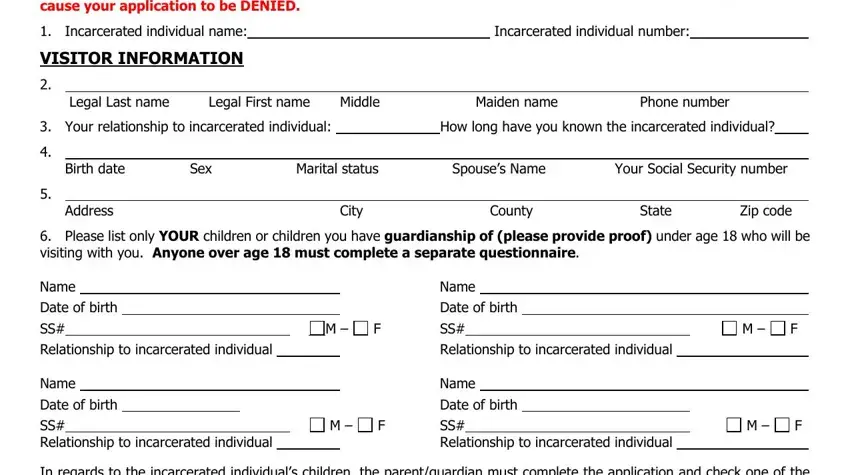
NOTICE: Before completing this application, please review the Department of Corrections search procedures on the back of this application. DO NOT LEAVE BLANKS OR PROVIDE FALSE INFORMATION. Doing so will cause your application to be DENIED.
1. |
Incarcerated individual name: |
|
|
|
Incarcerated individual number: |
|
|
VISITOR INFORMATION |
|
|
|
|
|
|
|
|
|
2. |
|
|
|
|
|
|
|
|
|
|
|
|
Legal Last name |
Legal First name |
Middle |
Maiden name |
Phone number |
|
|
3. |
Your relationship to incarcerated individual: |
|
How long have you known the incarcerated individual? |
4. |
|
|
|
|
|
|
|
|
|
|
|
|
Birth date |
Sex |
Marital status |
Spouse’s Name |
Your Social Security number |
5. |
|
|
|
|
|
|
|
|
|
|
|
|
Address |
|
|
|
City |
|
County |
State |
Zip code |
6.Please list only YOUR children or children you have guardianship of (please provide proof) under age 18 who will be visiting with you. Anyone over age 18 must complete a separate questionnaire.
Name |
|
|
|
|
|
Name |
|
|
|
Date of birth |
|
|
|
|
|
Date of birth |
|
|
|
SS# |
|
M – |
F |
SS# |
M – |
F |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Relationship to incarcerated individual |
|
|
|
|
|
Relationship to incarcerated individual |
|
|
|
Name |
|
|
|
|
|
Name |
|
|
|
Date of birth |
|
|
|
|
|
|
Date of birth |
|
|
|
SS# |
|
|
|
M – |
F |
SS# |
M – |
F |
|
|
|
|
|
|
|
|
|
|
|
Relationship to incarcerated individual |
|
|
|
|
|
Relationship to incarcerated individual |
|
|
|
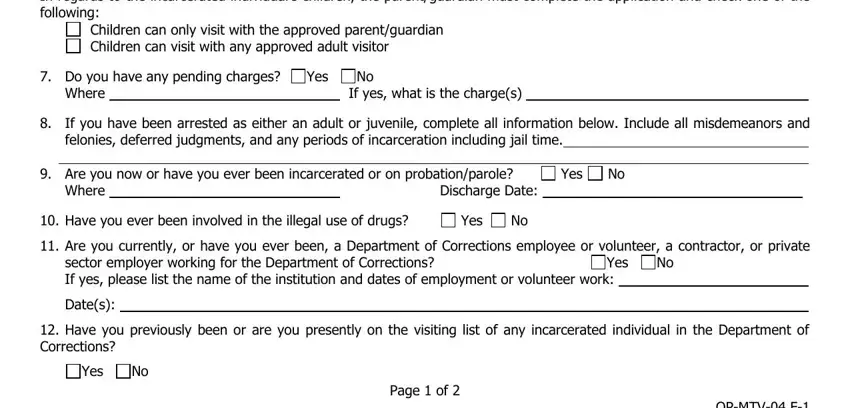
In regards to the incarcerated individual’s children, the parent/guardian must complete the application and check one of the following:
Children can only visit with the approved parent/guardian Children can visit with any approved adult visitor
7. Do you have any pending charges? |
Yes |
No |
Where |
|
|
If yes, what is the charge(s) |
8.If you have been arrested as either an adult or juvenile, complete all information below. Include all misdemeanors and felonies, deferred judgments, and any periods of incarceration including jail time.
9. |
|
Are you now or have you ever been incarcerated or on probation/parole? |
Yes |
No |
|
|
Where |
|
|
Discharge Date: |
|
|
|
10. |
Have you ever been involved in the illegal use of drugs? |
Yes |
No |
|
|
|
11. Are you currently, or have you ever been, a Department of Corrections employee or volunteer, a contractor, or private
sector employer working for the Department of Corrections? Yes No If yes, please list the name of the institution and dates of employment or volunteer work:
Date(s):
12.Have you previously been or are you presently on the visiting list of any incarcerated individual in the Department of Corrections?
Yes No
Page 1 of 2
OP-MTV-04 F-1
13. Have your visitation privileges ever been denied, suspended, or terminated? |
Yes |
No |
14.If you answered “yes” to either of the two above questions, please list incarcerated individual’s name, number and your relationship to him/her:
15.To enhance your safety as a visitor, please let us know if you have been the victim of an incarcerated individual supervised/incarcerated by the IDOC. If so, please list the incarcerated individual (s) name, ID number (if known), county, charge and case number:
16. Are you a legal citizen of the United States (you will be required to show a picture ID to visit). |
Yes |
No |
NOTICE: The Department of Corrections will evaluate this information against state and federal law enforcement databases. Failure to accurately complete any of the above information will result in rejection of this application. Please ensure that you sign the back page of the application. You are advised to keep a copy of this application
NOTICE:
All visitors are subject to search procedures: This may include non-intrusive electronic search methods. If a visitor refuses to be searched, you will not be permitted to visit and your visiting privileges may be revised.
In order to maintain drug-free prison zones, the non-intrusive ION SCAN method of detecting the use of, handling of or association with illegal substances (drugs) may be applied to prospective visitors. Should this test provide a positive indication of illegal substance association or you refuse to be tested, the following minimum visiting restrictions shall apply:
A)First Occurrence. Visiting privileges will be suspended from the date and time of the test for the next two (2) visiting days. Future visits may be restricted to non-contact status.
B)Second Occurrence. Visiting privileges will be suspended from the date and time of the test for the next seven (7) visiting days. Future visits may be restricted to non-contact status.
C)Third Occurrence. Visiting privileges will be suspended from the date and time of the test for the next fifteen (15) visiting days. Future visits may be restricted to non-contact status.
D)Fourth Occurrence. Visiting privileges will be suspended from the date and time of the test for the next thirty (30) visiting days. In addition, you will be placed on non-contact visit status for one hundred and eighty (180) days from the date of the first eligible visit. If you test positive from this date forward, visiting privileges may be permanently restricted to non-contact status.
E)Refusal to submit to being tested will suspend visiting privileges to the facility for fifteen (15) calendar days from the time of refusal.
Visitors may send a written appeal to the Warden regarding receipt of any of the above sanctions.
I hereby give my consent to initiate a background investigation with law enforcement agencies and authorize law enforcement agencies to furnish information. I also understand any falsification of the information I provided above will disqualify me from visiting.
17.
It is the responsibility of the incarcerated individual to notify you of visitor application approval.
Return completed application to Centralized Visiting Authority to: |
Mt. Pleasant Correctional Facility |
|
Attn: Central Records |
|
1200 E. Washington |
cc: file |
Mt. Pleasant, IA 52641 |
|
BREAK THE SILENCE -- Iowa DOC has a zero tolerance for sexual violence of any kind. If you are told about or are concerned about sexual violence committed against any person in an IDOC prison, please contact the Warden immediately.
Revised: Oct. 2000, Sept. 2006, June 2007, Feb. 2008. Reviewed: Feb. 2009. Revised: July 2010. Reviewed: Jan. 2011, May
2012. Revised: Nov. 2013, Oct. 2014, July 2015, April 2016. Reviewed: April 2017. Revised: April 2019. Page 2 of 2
OP-MTV-04 F-1