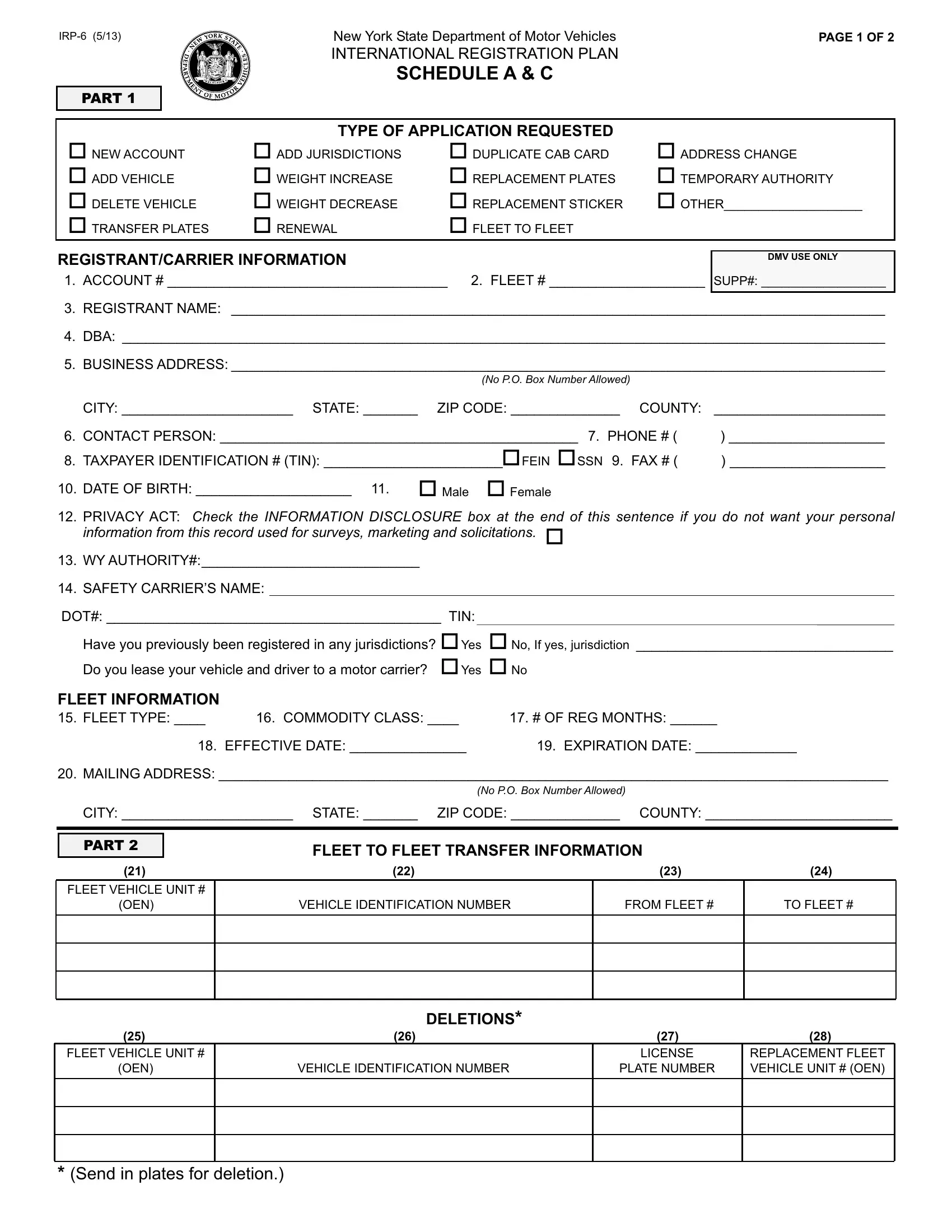
Navigating the complexities of vehicle registration, especially for commercial vehicles operating across multiple jurisdictions, requires familiarity with specific forms like the IRP-6 form provided by the New York State Department of Motor Vehicles. This form is essential for truckers, fleet operators, and commercial vehicle owners who are part of the International Registration Plan (IRP), facilitating the registration of vehicles that travel interstate. The IRP-6 form covers a wide array of applications, including new accounts, fleet additions, vehicle deletions, address changes, and more, ensuring that all relevant vehicle and owner information is accurately recorded and updated. From assigning account and fleet numbers to specifying the type of application requested—be it for new registrations, renewal, weight changes, or temporary authority—the form is comprehensive. It also gathers detailed vehicle data, owner information, and operational specifics crucial for compliance with the IRP's apportioned registration requirement. By completing this form, registrants can ensure their vehicles are legally authorized to operate across state lines, carrying goods or passengers, with the correct weight limits and information disclosed to relevant jurisdictions. The form also addresses privacy concerns and includes a section for disclosing personal information protection preferences. Moreover, it requires certification by the applicant affirming the accuracy of the provided information and compliance with the New York State Vehicle and Traffic Law, underscoring the legal responsibility borne by carriers to ensure their fleets meet all regulatory standards.
| Question | Answer |
|---|---|
| Form Name | IRP-6 Form |
| Form Length | 2 pages |
| Fillable? | Yes |
| Fillable fields | 180 |
| Avg. time to fill out | 36 min 34 sec |
| Other names | OEN, irp6 form download pdf, irp6 template, irp6 form pdf |
New York State Department of Motor Vehicles |
PAGE 1 OF 2 |
||
|
INTERNATIONAL REGISTRATION PLAN |
|
|
|
SCHEDULEA& C |
|
|
PART 1 |
|
|
|
|
TYPE OFAPPLICATION REQUESTED |
|
|
NEWACCOUNT |
ADD JURISDICTIONS |
DUPLICATE CAB CARD |
ADDRESS CHANGE |
ADD VEHICLE |
WEIGHT INCREASE |
REPLACEMENT PLATES |
TEMPORARYAUTHORITY |
DELETE VEHICLE |
WEIGHT DECREASE |
REPLACEMENT STICKER |
OTHER____________________ |
TRANSFER PLATES |
RENEWAL |
FLEET TO FLEET |
|
REGISTRANT/CARRIER INFORMATION |
|
DMV USE ONLY |
|
|
|
||
1. ACCOUNT # ____________________________________ |
2. FLEET # ____________________ SUPP#: __________________ |
||
3.REGISTRANT NAME: ____________________________________________________________________________________
4.DBA: __________________________________________________________________________________________________
5.BUSINESSADDRESS:____________________________________________________________________________________
|
|
(No P.O. Box NumberAllowed) |
|
|
CITY: ______________________ STATE: _______ |
ZIP CODE: ______________ COUNTY: |
______________________ |
6. |
CONTACT PERSON: ______________________________________________ 7. PHONE # ( |
) ____________________ |
|
8. |
TAXPAYER IDENTIFICATION # (TIN): _______________________FEIN SSN 9. FAX # ( |
) ____________________ |
|
10. |
DATE OF BIRTH: ____________________ 11. |
Male Female |
|
12.PRIVACY ACT: Check the INFORMATION DISCLOSURE box at the end of this sentence if you do not want your personal information from this record used for surveys, marketing and solicitations.
13.WYAUTHORITY#:____________________________
14.SAFETY CARRIER’S NAME:
DOT#: ___________________________________________ TIN: |
|
|||
|
Have you previously been registered in any jurisdictions? Yes |
No, If yes, jurisdiction _________________________________ |
||
|
Do you lease your vehicle and driver to a motor carrier? |
Yes No |
||
FLEET INFORMATION |
|
|
|
|
15. |
FLEET TYPE: ____ |
16. COMMODITY CLASS: ____ |
17. # OF REG MONTHS: ______ |
|
|
18. EFFECTIVE DATE: _______________ |
19. EXPIRATION DATE: _____________ |
||
20. |
MAILINGADDRESS: ______________________________________________________________________________________ |
|||
|
|
|
(No P.O. Box NumberAllowed) |
|
|
CITY: ______________________ STATE: _______ |
ZIP CODE: ______________ COUNTY: ________________________ |
||
|
|
|
|
|
PART 2
FLEET TO FLEET TRANSFER INFORMATION
(21) |
(22) |
(23) |
(24) |
FLEET VEHICLE UNIT #
(OEN)
VEHICLE IDENTIFICATION NUMBER
FROM FLEET #
TO FLEET #
DELETIONS*
(25) |
(26) |
(27) |
(28) |
FLEET VEHICLE UNIT #
(OEN)
VEHICLE IDENTIFICATION NUMBER
LICENSE |
REPLACEMENT FLEET |
PLATE NUMBER |
VEHICLE UNIT # (OEN) |
|
|
*(Send in plates for deletion.)
PART 3
WEIGHT
INFORMATION Account # ____________________________________
29.Please list the weight you want on your cab card for the jurisdictions you intend to travel through. Canadian jurisdictions will print the weight in kilograms on the cab card.
AK |
____________________ |
KS |
____________________ |
NJ |
____________________ |
VT |
____________________ |
|
|
AL |
____________________ |
KY |
____________________ |
NM |
____________________ |
WA |
____________________ |
|
|
AR |
____________________ |
LA |
____________________ |
NV |
____________________ |
WI |
____________________ |
|
|
AZ |
____________________ |
MA |
____________________ |
NY |
____________________ |
WV |
____________________ |
|
|
CA |
____________________ |
MD |
____________________ |
OH |
____________________ |
WY |
____________________ |
|
|
CO |
____________________ |
ME |
____________________ |
OK |
____________________ |
AB |
____________________ (Canada) |
||
CT |
____________________ |
MI |
____________________ |
OR |
____________________ |
BC |
____________________ (Canada) |
||
DC |
____________________ |
MN |
____________________ |
PA |
____________________ |
MB |
____________________ (Canada) |
||
DE |
____________________ |
MO |
____________________ |
RI |
____________________ |
NB |
____________________ (Canada) |
||
FL |
____________________ |
MS |
____________________ |
SC |
____________________ |
NL |
____________________ (Canada) |
||
GA |
____________________ |
MT |
____________________ |
SD |
____________________ |
NS |
____________________ (Canada) |
||
IA |
____________________ |
NC |
____________________ |
TN |
____________________ |
ON |
____________________ (Canada) |
||
ID |
____________________ |
ND |
____________________ |
TX |
____________________ |
PE |
____________________ (Canada) |
||
IL |
____________________ |
NE |
____________________ |
UT |
____________________ |
QC |
____________________ (Canada) |
||
IN |
____________________ |
NH |
____________________ |
VA |
____________________ |
SK |
____________________ (Canada) |
||
|
|
|
VEHICLE INFORMATION FOR NEWACCOUNTS ORADDITIONS |
|
|
||||
|
PART 4 |
|
|
|
|||||
30.VEHICLE #1:
A) VEHICLE IDENTIFICATION NUMBER |
|
|
|
B) YEAR |
C) |
MAKE |
D) VEHICLE TYPE |
E) FUEL/CYL |
F) WHEELBASE |
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
G) UNLADEN WT |
H) SEATS |
I) COMBINED |
|
J) COLOR |
K) OWNER NAME |
|
|
|
|
|
|||||
|
|
/AXLES |
AXLES |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
L) TITLE DOC # |
|
M) TITLE DOC. JUR. |
N) SAFETY TAXPAYER ID # (TIN) |
FEIN SSN |
|
O) SAFETY US DOT # |
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
P) Vehicle Safety responsibility will change |
Q) SAFETYNAME |
|
|
|
|
|
|||||||||
during the year? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Yes |
No |
|
|
|
|
|
|
|
|
|
|
||
R) FLEET VEHICLE # (OEN)
S)MAXIMUM DESIRED WEIGHT
T)PURCHASE PRICE
U)PURCHASE DATE
V) FACTORY PRICE |
W)INS. CO. CODE |
X) CURRENT PLATE # |
Y) CURRENT PLATE CLASS |
Z) SPECIAL USE |
|
|
|
|
|
REGISTRATION |
IF THE REGISTRANT IS NOT THE OWNER, fill in the information below. Proof of ownership, and proof of the |
|||||||
AUTHORIZATION |
OWNER’S name and date of birth, are required. |
|
|
|
|
|
|
|
Vehicle #1 - Owner’s Name |
|
Date of Birth |
|
Is the vehicle leased? |
||||
|
|
|
|
|
|
|
Yes No |
|
Address |
Apt. No. |
City |
State |
Zip Code |
||||
|
|
|
|
|
|
|
|
|
The person named in number 3 of Part 1 is authorized to register this vehicle in his/her name. |
|
|
|
|
|
|||
Owner’sAuthorized |
|
|
|
|
|
|
|
|
Signature - |
|
|
|
|
Date: |
|
|
|
|
|
|
|
|
|
|
||
Ifsigningforacorporation,printyourfullnameandtitlehere
CERTIFICATION: I, the Undersigned, certify under penalty of perjury that all information provided in thisApplication is true and accurate to the
best of my knowledge, and that the subject vehicle: is fully equipped, inspected, insured, and will be operated, in compliance with NewYork State Vehicle and Traffic Law (VTL); possesses a valid NYS inspection issued within the last twelve (12) months; or, in the alternative, has qualified for an extension of such inspection (see, DMV form
IMPORTANT: By signing thisApplication, the Undersigned acknowledges that intentionally making a false statement on this form is a misdemeanor underVTLSection392,andmayresultincriminalprosecution,aswellassuspensionorrevocationoftheregistrationofthesubjectvehicle.
Name ofApplicant/Business Entity (please print):
Sign here:- |
|
|
|
|
|
|
Title: |
|
|
Date (mm/dd/yyyy): |
/ |
/ |
|
|
|
|
|
|
|
|
|
|
If signing as agent for a business entity, write your title (CEO, President, |
|
|||
|
|
Anyone else signing as agent for a business entity must send in an original Power ofAttorney. |
|
|
||
|
|
|
PAGE 2 OF 2 |
|||