

Handling PDF forms online is always quite easy with this PDF tool. You can fill in scisp 2507 super here painlessly. Our tool is continually evolving to provide the very best user experience possible, and that is thanks to our resolve for continuous enhancement and listening closely to feedback from users. Here's what you'll want to do to get going:
Step 1: Access the PDF form in our tool by hitting the "Get Form Button" at the top of this page.
Step 2: With our handy PDF editing tool, you'll be able to do more than simply complete blanks. Edit away and make your docs appear high-quality with customized text put in, or tweak the file's original content to perfection - all that comes along with the capability to incorporate your own graphics and sign the PDF off.
In order to finalize this PDF document, ensure that you provide the necessary details in every single area:
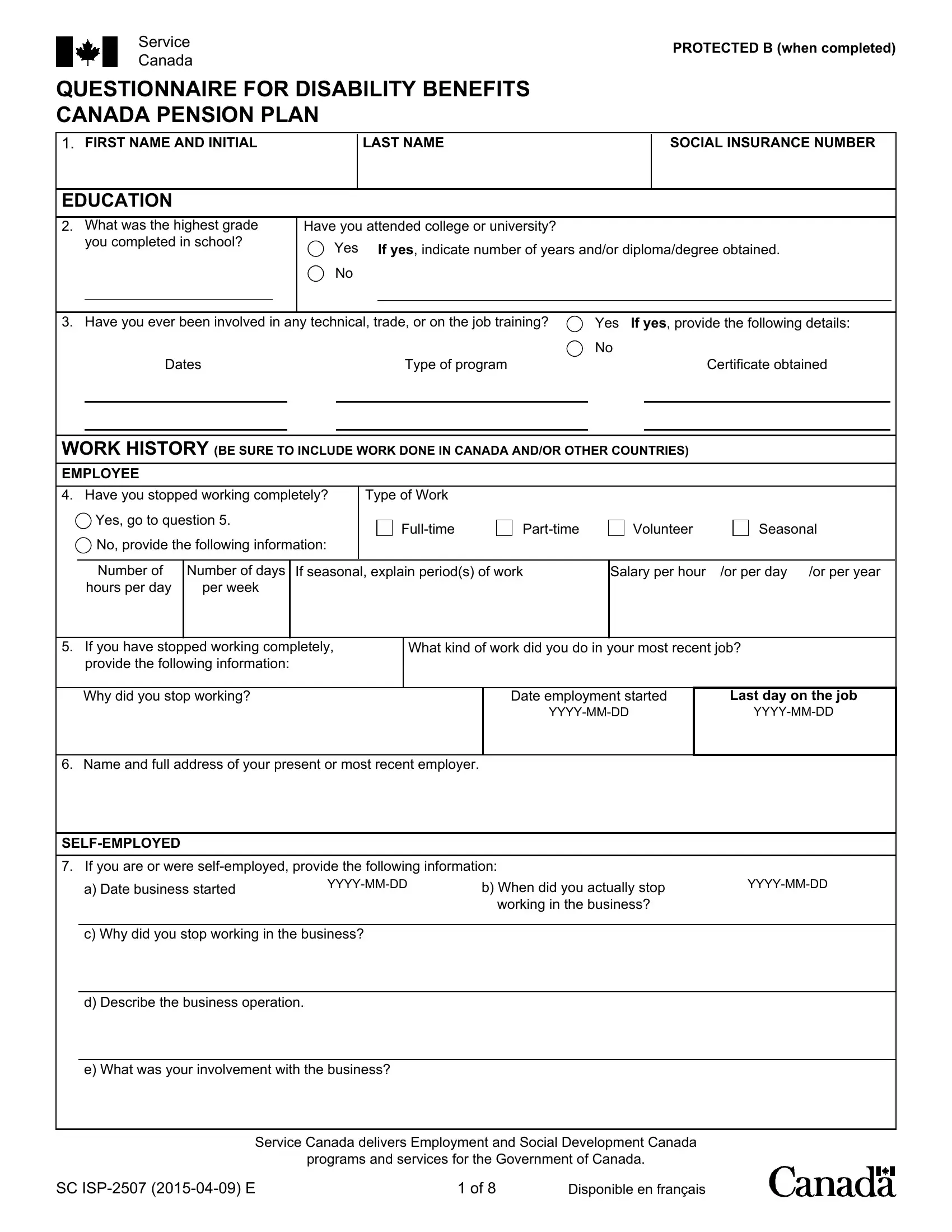
1. For starters, once completing the scisp 2507 super, start in the area containing next blank fields:
2. After this selection of blank fields is done, go on to enter the applicable details in all these - Number of hours per day, Number of days per week, If seasonal explain periods of work, Salary per hour, or per day, or per year, If you have stopped working, Why did you stop working, What kind of work did you do in, Date employment started, Last day on the job, YYYYMMDD, YYYYMMDD, Name and full address of your, and SELFEMPLOYED.
As to or per day and YYYYMMDD, ensure that you do everything properly here. These two are thought to be the most important fields in the PDF.
3. Completing e What was your involvement with, Service Canada delivers Employment, programs and services for the, SC ISP E, and Disponible en français is essential for the next step, make sure to fill them out in their entirety. Don't miss any details!
4. It is time to start working on this fourth form section! In this case you will have all of these Social Insurance Number, PROTECTED B when completed, SELFEMPLOYED CONTINUED, f Are you involved in the business, Yes explain your present, No provide the following, Indicate what disposition has been, sold, rented, profit sharing, Date of disposition YYYYMMDD, If no disposition has been made of, g What was the last year that an, on the operation of the business, and OTHER WORK HISTORY fields to fill out.
5. Since you approach the last sections of your form, there are actually several more things to complete. Specifically, IF THERE IS INSUFFICIENT SPACE TO, In the past two years did you do, Yes If yes provide the following, Type of work, Number of hours, Number of hours, per day, per week, Work started YYYYMMDD, Last day on the job, YYYYMMDD, Name and full address of employer, Have you done any other type of, Yes If yes list the type of work, and From should be filled in.
Step 3: When you've glanced through the details you given, click on "Done" to complete your FormsPal process. Create a 7-day free trial option with us and obtain immediate access to scisp 2507 super - which you'll be able to then begin to use as you want from your FormsPal account. We do not sell or share any details you enter when working with documents at our website.