
It's an easy task to complete the jackson life insurance company forms empty blanks. Our PDF tool will make it pretty much effortless to complete any type of PDF file. Down below are the only four steps you should take:
Step 1: The following website page has an orange button saying "Get Form Now". Hit it.
Step 2: As you get into the jackson life insurance company forms editing page, you will find all the functions you can undertake with regards to your document at the upper menu.
Feel free to provide the next information to prepare the jackson life insurance company forms PDF:
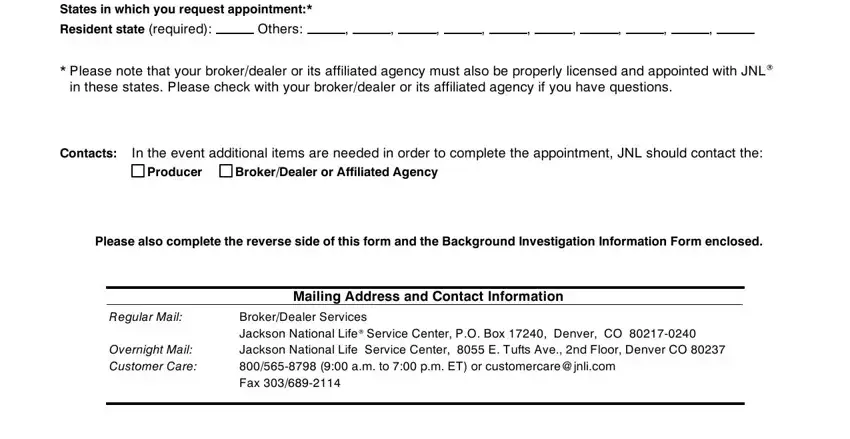
Complete the States, in, which, you, request, appointment Resident, state, required Others, Contacts, Producer, Broker, Dealer, or, Affiliated, Agency Mailing, Address, and, Contact, Information Regular, Mail and Overnight, Mail, Customer, Care fields with any data which may be asked by the program.
You'll be required to write down the details to help the application prepare the section Disclosure, and, Consent
In the field Printed, Name Signature, and Date, mm, dd, yyyy identify the rights and obligations of the parties.
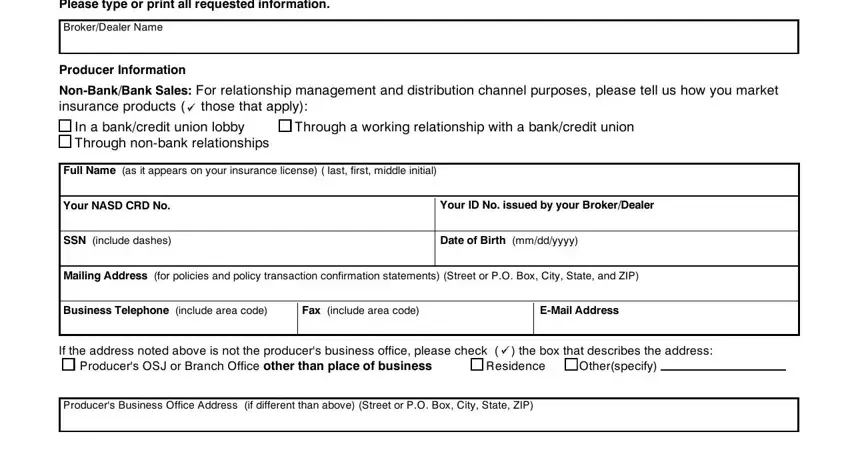
Review the sections Producer, Name S, SN, included, ashes From, mm, dd, yyyy to, mm, dd, yyyy From, mm, dd, yyyy to, mm, dd, yyyy From, mm, dd, yyyy to, mm, dd, yyyy Yes, Yes, Yes, and you and then complete them.
Step 3: Press the Done button to save your form. At this point it is at your disposal for upload to your electronic device.
Step 4: Prepare a copy of every single document. It's going to save you time and allow you to stay away from complications in the long run. Keep in mind, the information you have isn't going to be revealed or analyzed by us.
