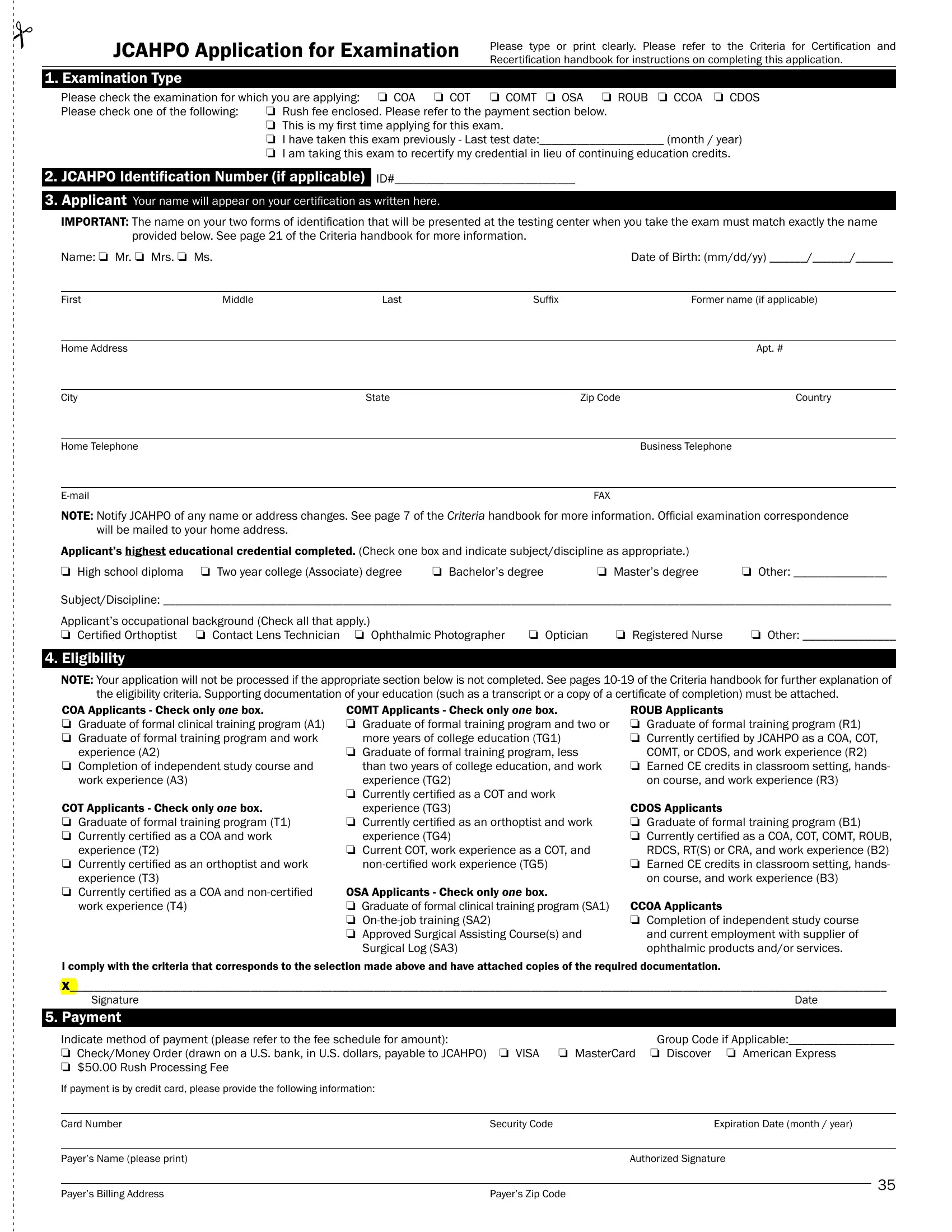
The journey toward certification in the ophthalmic medical field is marked by an essential step: filling out the JCAHPO Application for Examination form. This meticulously designed form serves as the gateway for professionals aiming to validate their expertise across various specialties, including Certified Ophthalmic Assistant (COA), Certified Ophthalmic Technician (COT), and several others, through the Joint Commission on Allied Health Personnel in Ophthalmology (JCAHPO). Applicants are instructed to fill out the form with precise details such as examination type, personal identification, educational background, and employment information, ensuring the accuracy to match the identification presented at testing centers. The application delves into eligibility criteria linked to educational and occupational background, requiring supporting documentation for verification. Furthermore, it outlines payment methods, underscoring the option for expedited processing and highlights the responsibility agreement that underscores ethical conduct and respect for confidential examination content. With a focus on compliance with the Americans with Disabilities Act (ADA), the form also accommodates candidates requiring special examination conditions, ensuring inclusivity. Prospective candidates are guided to complete the application with attention to verifying their eligibility, securing a sponsor or employer endorsement, and fulfilling specific prerequisites for their targeted certification. The process concludes with an agreement towards maintaining the integrity of the certification pursuit, emphasizing the form’s pivotal role in the journey toward achieving and maintaining professional certification in the ophthalmic field.
| Question | Answer |
|---|---|
| Form Name | Jcahpo Application For Examination Form |
| Form Length | 4 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 1 min |
| Other names | Ophthalmic, ADA, Orthoptist, OSA |